Download
1 / 33
330 likes | 597 Views
VEGF targeted therapy in NET: When to give, whom to give!. Diane Reidy Lagunes Memorial Sloan Kettering Cancer Center December 3, 2011.

E N D
VEGF targeted therapy in NET: When to give, whom to give! Diane ReidyLagunes Memorial Sloan Kettering Cancer Center December 3, 2011
Notre Dame(5-0-0) and Ohio State (4-0-0) met at Columbus before a crowd of 80,000. Grantland Rice described what happened: "Completely outplayed in the first two quarters, trailing 13 to 0 as the final quarter started with every killing break against it-- breaks that would crack the heart of an iron ox-- this Notre Dame team came surging back in the final quarter...". Notre Dame scored early in the fourth, but the extra point attempt bounced off the crossbar, and it was 13-6. After an interception, the Irish drove to within six inches of the goal line when Milner fumbled the ball away. With 90 seconds left, Andy Pilney passed to Mike Layden for a touchdown, but the extra point failed and the Irish trailed 13-12. Andy Pilney forced a Buckeye fumble at midfield, giving the Irish the ball at the 49 yard line, and on the next play, Pilney, taking back over as quarterback, scrambled to the 19 yard line, but was injured. With only one play left in the game, reserve quarterback Bill Shakespeare passed to Wayne Milner for the 18-13 win “ November 2, 1935
Histological Classification of Neuroendocrine Tumors (NETs) ENETS, European Neuroendocrine Tumor Society; WHO, World Health Organization; HPF, high-power fields. POORLY DIFFERENTIATED NE CARCINOMAS ARE MANAGED WITH PLATINUM BASED THERAPY AND ARE CONSIDERED AGGRESSIVE CANCERS. THEY WILL NOT BE FURTHER DISCUSSED TODAY.
Well Differentiated Neuroendocrine Tumors Uncommon cancers most commonly found in the aerodigestive tract If primary location is in pancreas -> pancreatic NET (formerly known as islet cell carcinoma) If primary location is outside the pancreas -> carcinoid tumor
Does the location of primary tumor matter and if so, why? YES Genetics are different as are responses to therapy
Mutations in pNETsJiao, et al Science 2011 • MEN-1 gene, 44%; • DAXX 25%; ATRX 17%, • mTOR pathway 14%(PTEN, TSC2, PIK3CA) mTOR regulates production of angiogenic growth factors and the proliferation of vascular endothelial cells
NETs are hypervascular Larry Schwartz, MD
Nonsurgical Liver-Directed TherapyTargeting VEGF at a “Macro” Level • Bland and Chemoembolization: objective response rates > 50%; median survival up to 15-80 months; high incidence of post-embolization syndrome • Yttrium-90 radioembolization: objective response rates >50%; median survival 14-70 months; long-term toxicities remain unknown • NO RANDOMIZED DATA comparing the different techniques and, therefore, no data to know which technique is more effective • R01 submitted MSKCC Randomized Phase II Bland versus SIRTs Liu DM, et al. Am J Clin Oncol. 2009;32(2):200-215.
VEGF and VEFR in NET at a “Micro” level • Angiogenic growth factors contribute to tumor growth • VEGF is found in 84% of carcinoid and 59% of pancreatic NETs • VEGFR is found in 71% of carcinoid and 67% of pancreatic NETs • Suggests autocrine stimulation in carcinoid and pancreatic NETs Hobday et al. Proc ASCO. 2003;22:269. Abstract 1078.
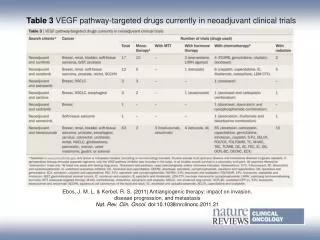
Medical Treatment Outlook for Advanced Carcinoid in 2011 Somatostatin Analogue Disease Progression Functional (Carcinoid Syndrome) Investigational Agents Regional Therapy Carcinoid Observation Nonfunctional Midgut Octreotide LAR (PROMID)
Randomized Phase II Study of Bevacizumab vs Interferon in Advanced Carcinoid 41 patients Bev 15 mg/kg q 3 wks +octreotide X 18 wks PEG interferon alpha 2B q +octreotide X 18 wks Bevacizumab + PEG interferon ORR= 18% Bev Yao, J. C., et al J ClinOncol. 2008 Mar 10;26(8):1316-23.
VEGF and VEGFr Inhibitors • Bevacizumab 15 mg/kg q 21 days: ORR 18% carcinoid • Sorafenib-400 mg bid • Response in 4 of 41 carcinoid patients (10%) • Response in 4 of 41 pancreatic NETs (10%) • 43% grade 3-4 toxicity • Sunitinib50 mg daily, 4 of 6 weeks: • Response in 11 of 66 pancreatic NETs (17%) • Response in 1 of 41 (2%) carcinoid tumors • 25% of patients developed grade 3 fatigue. Yao, J. C., et al J ClinOncol. 2008 Mar 10;26(8):1316-23. Kulke, et al J Clin Oncol. 2008 Jul 10;26(20):3403-10. Hobday et al ASCO 2007 Vol 25, No. 18S
Maximum % Reduction of Target Lesions by Patient: Phase II Study of Sunitinib in NET Carcinoid 40 20 0 20 40 60 80 100 Percentage (%) pNET 40 20 0 20 40 60 80 100 Partial responders by RECIST
Poor prognosis (N = 283) Carcinoid: SWOG 0518 Phase III Study Octreotide + interferon R Supported by CTSU Endorsed by ECOG, CALGB, NCCTG Octreotide + bevacizumab CALGB, Cancer and Leukemia Group B; CTSU, Cancer Trials Support Unit; ECOG, Eastern Oncology Cooperative Group; NCCTG, North Central Cancer Treatment Group; SWOG, Southwestern Oncology Group.
Medical Treatment Outlook for Advanced Pancreatic NETs in 2011 Somatostatin Analog Disease Progression Functional Nonfunctional, Stable Disease, or Low Volume Expectant Management Investigational Agents Regional Therapy pNET Somatostatin Analog Everolimus Nonfunctional and Disease Growth with Symptoms or High Volume Disease Sunitinib Chemotherapy* *Generally for high tumor burden pNET, pancreatic neuroendocrine tumor.
Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors E. Raymond and Others | N Engl J Med 2011;364:501-513 Everolimus for Advanced Pancreatic Neuroendocrine Tumors J.C. Yao and Others | N Engl J Med 2011;364:514-523
Sunitinib – Phase III Trial Design Eligibility criteria: Well-differentiated, malignant pancreatic endocrine tumor Radiologic documentation of progressive disease within 12 months of randomization Not amenable to treatment with curative intent Sunitinib 37.5 mg PO daily, continuous daily dosing RANDOMIZE N = 340 (planned) N = 171 (actual) Final analysis planned at 260 events; one interim analysis planned at 130 events 1:1 Placebo Multiphasic CT or MRI performed every 12 weeks Primary endpoint: progression-free survival Secondary endpoints: OS, ORR, TTR, duration of response, safety, patient-reported outcomes Raymond E, et al. N Engl J Med. 2011;364(6):501-513.
Sunitinib Phase III TrialProgression-Free Survival and ORR Progression-Free Survival 11.5 months vs 5.5 months ORR, objective response rate; CR/PR, complete response/partial response; SD, stable disease, PD, progressive disease. Raymond E, et al. N Engl J Med. 2011;364(6):501-513.
Sunitinib Phase III TrialSafety and Quality of Life Overall no difference in quality of life Quality of life worse in patients on sunitinib with diarrhea Raymond E, et al. N Engl J Med. 2011;364(6):501-513.
A prospective, multi-institutional phase II study of GW786034 (pazopanib) and depot octreotide (sandostatin LAR) in advanced low/intermediate grade neuroendocrine tumor (LGNET) Alexandria T. Phan1, James C. Yao1, David R. Fogelman1, Kenneth R. Hess1, Chaan S. Ng1, Susie A. Bullock1, Paige Malinowski2, Eileen Regan2, and Matthew H. Kulke2 1University of Texas M. D. Anderson Cancer Center 2Dana-Farber Cancer Institute ASCO 2010 Abstract 4001
STOP Cont to 30 pts STOP Cont to 30 pts Patients with carcinoid/pNET • ECOG 0-1 • Low / intermediate grade • Stable dose octreotide > 2 mo • No prior anti-VEGF or anti-VEGFR • < 1 prior cytotoxic therapy Pazopanib 800 mg PO daily + cont depot octreotide Pazopanib 800 mg PO daily + cont depot octreotide Carcinoid pNET Study design Parallel phase II study Two stage design with early termination for no activity Yes No At 20 pts 1 of 20 CR/PR? Yes 3 of 20 CR/PR? At 20 pts Weeks No Primary Objective: ORRSecondary Objectives: PFS and Optional functional CT Response evaluation 0 12 24 36 48 Phan et al, ASCO 2010
Results – EfficacyRECIST best protocol response: By intention to treat *minor response, not PR but > 15%; #are confirmed; ^non-evaluable for responses Phan et al, ASCO 2010
What about investigational studies combining VEGF inhibitors?
Combination Approaches With Bevacizumab • Phase II XELOX + bevacizumab (N = 40; n = 31 evaluable for response)1 • Partial response: 7 patients (23%); 6 had pancreatic NETs and 1 had an unknown primary with liver involvement • Stable disease: 22 patients (71%) • Progressive disease: 2 patients (6%) • Progression-free survival rate at 1 year: 52% • Median progression-free survival: 13.7 months • Phase II FOLFOX + bevacizumab in advanced progressive NET (N = 13; n = 11 evaluable for response)2 • Best radiologic response to therapy by RECIST 1Kunz P, et al. J Clin Oncol. 2010;28(15S). Abstract 4104. 2Bergsland EK, et al. J Clin Oncol. 2008;26(15S). Abstract 216.
Summary Courtesy of Dietmar Tamandl, MD
Can we combine VEGF and mTOR?mTOR (Temsirolimus) + VEGF (Bevacizumab)PI: Manisha Shah, MD (Carcinoid Cohort); Tim Hobday (pNETCohort) • Trial in collaboration with the Mayo Clinic, OSH, and CTEP pNETabstract, GI ASCO, 2012
Everolimus and Octreotide With or Without Bevacizumab in Treating Patients With Locally Advanced or Metastatic Pancreatic Neuroendocrine Tumors That Cannot Be Removed By Surgery PI: Matt Kulke CALGB NCT01229943
Conclusions • When to Give in 2011? • UPON PROGRESSION IN PATIENTS WITH PANCREATIC NETS; SUTENT IS THE ONLY VEGF TARGETED AGENT FDA APPROVED • Whom to Give in 2011? • PATIENTS WITH PROGRESSIVE PANCREATIC NETS • Promising activity with bevacizumab in phase II study for carcinoids; phase III trial on going • Combination bev/mTOR in early studies ongoing
Conclusions Continued • Sunitinibis not approved for extra-pancreatic (ie, carcinoid) tumors • Side effects of sunitinib are predictable but can impair out patient’s quality of life • Ongoing trials with correlative studies (radiographic and biologic) are critical in allowing us to understand the role of VEGF in this tumor type