Download
1 / 37
790 likes | 2.51k Views
Bronchopulmonary Dysplasia . John Salyer RRT-NPS, MBA, FAARC Director Respiratory Therapy Seattle Children’s Hospital and Research Institute. A Little History. Originally described by Northway in 1967 Report of a series of 32 patients in NEJM, average gestational age 32 weeks

E N D
Bronchopulmonary Dysplasia John Salyer RRT-NPS, MBA, FAARC Director Respiratory Therapy Seattle Children’s Hospital and Research Institute
A Little History Originally described by Northway in 1967 • Report of a series of 32 patients in NEJM, average gestational age 32 weeks • All were treated with 100% oxygen, then prolonged mechanical ventilation with 80-100% oxygen • Before mechanical ventilation was available the usual course of RDS was several days of severe lung disease to which the infant either succumbed or recovered completely in 7-10 days
History (cont.) • The addition of mechanical ventilation led to appearance of a new syndrome • Stage I, days 1-3, HMD (RDS) • Stage II, days 4-10, opacification of lungs, with bronchiolar and alveolar necrosis • Stage III, days 10-20, transition to a CXR with a reticular network of small rounded areas of radiolucency, emphysematous and atelectatic airspaces, with pulmonary fibrosis • Stage IV, hyperexpanded and cystic lungs. cor pulmonale
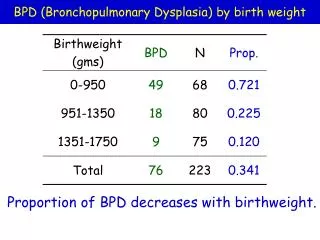
Definition • Shennan noted that if oxygen requirement at 36 weeks used as threshold over 50% of infants would have abnormal pulmonary follow-up (Shennan, 1988) • Now usually defined as requirement for supplemental oxygen at: • 36 weeks postmenstrual age if born at or before 32 weeks’ gestational age • 4 weeks of age if born after 32 weeks’ gestational age
Physiologic Test • BPD if at 35-37 weeks post menstrual age: • receiving mechanical ventilation, or • CPAP, or • >30% oxygen with saturation <96% • If infant is receiving <30% oxygen or ≥30% oxygen with saturation >96% then: • Wean O2 to room air • No BPD if saturation > 90% in room air for 30 minutes
Pathology Classic BPD • Airway injury • Epithelial metaplasia with type II cell hyperplasia • Smooth muscle hypertrophy • Parenchymal fibrosis, alternating with emphysema • Capillary dysplasia
Low power view of lung from infant who died from BPD at 2.5 months of age. Note alternating areas of emphysema and atelectasis, and strands of fibrosis.
Preterm spontaneously breathing lambs supported with N-HFV or intubation/MV (n=16) N-HFV group had greater oxygenation (p<0.05) at a lower FiO2 and improved alveolarization
Histology of BPD Preterm spontaneously breathing lambs supported with N-HFV or intubation/MV (n=16) N-HFV group had greater oxygenation (p<0.05) at a lower FiO2 and improved alveolarization Albertine et al., Am J Respir Crit Care. 2008
Classic vs. New BPD • Much of the histologic findings of “old BPD” seen in animal models with oxygen toxicity • New epidemiology • Most common in ELBW infants • Risk factors: low gestational age, postnatal infection, maternal chorioamnionitis, PDA, mechanical ventilation • Some ELBW infants do not have RDS, with minimal early oxygen or mechanical ventilation
Clinical Presentation “New” BPD • Hazy lungs on CXR, with minimal cystic emphysema, or hyperinflation • Less airway reactivity • Less pulmonary hypertension (blue spells, “twits”) • Pathology • Minimal fibrosis, minimal airway injury • Decreased alveolar septation and microvascular development
Division of Respiratory Bronchioles • 20 to 32-36 weeks 3 generations of saccular septations, forming 524,000 respiratory bronchioles • Hypothesized that the further septation of respiratory bronchioles disrupted by inflammation/injury in new BPD
Pathology New BPDArrest of Alveolarization • Increased saccular diameters, fewer saccules (alveoli) • Collagen network disrupted, elastin not localized to fibers for secondary septation • No severe inflammation • Saccules lined with dysplastic type II cells • Seen in post-natal mice and rats exposed to inflammation or hyperoxia
Pathogenesis “New” BPD:Overview • Immaturity of structure and function before about 32 weeks’ gestation • Poorly developed airway supporting structures • Surfactant deficiency • Decreased compliance • Underdeveloped antioxidant mechanisms • Inadequate fluid clearance • Inflammation • Mechanical ventilation • Oxygen toxicity • Infection
Pathogenesis:Mechanical Injury • Over-distension of airways and airspaces (Volutrauma) • Excessively large tidal volumes, not pressure (Hernandez, 1989) • Association of decreased PCO2 with increased risk BPD (Garland, 1995) • Maximum end-inspiratory volume more important than tidal volume or FRC (Dreyfuss, 1993) • As few as 6 large manual inflations was enough to increase the lung damage premature lambs (Bjorklund, 1997) • Positive pressure causes bronchiolar lesions (Nilsson, 1978)
Pathogenesis:Oxygen Toxicity • Safe FiO2 level and duration are unknown • Cell damage from reactive oxygen metabolites • Cell enzyme inactivation • Preterm infants may have inadequate antioxidant defenses • Nutrient deficiencies • Immature enzyme development
Pathogenesis:Infection • Four-fold increase in BPD incidence with sepsis (Rojas, 1995) • Due to increased concentration of proinflammatory cytokines in amniotic fluid? • Association with Ureaplasma urealyticum (Hannaford, 1999) • Maternal chorioamnionitis associated with decreased RDS, but increased risk of BPD
Pathogenesis:Inflammation • Macrophages, lymphocytes, platelets in lung will release inflammatory mediators • Cytokines • Lipid mediators • Platelet factors (Ozdemir, 1997) • Complement activation • Increased vascular permeability • Protein leakage • Mobilization of neutrophils into interstitial and alveolar compartments • Release of reactive oxygen radicals, elastase, collagenase • Increased MIP-1 and IL-8, reduced IL-10 (Jobe 2001)
Sloughing bronchial epithelium Edema fluid Necrotic or Apoptotic Type I cell Inactivated surfactant Red cell Oxidants Activated neutrophil Leukotrienes Proteases Cellular debris TNF IL Hyaline membrane Fibrin Widened, edematous interstitium (interstitial pneumonia) Normal Alveolus Injured Alveolus (Acute Phase) Alveolar air space Type I cell Surfactant Layer Type II cell Interstitium Capillary Alveolar macrophage Red cell
Cardiopulmonary function in BPD • Decreased tidal volume • Increased airway resistance • Decreased dynamic lung compliance • Uneven airway obstruction • Gas trapping • Hyperinflation • Abnormal distribution of ventilation • Bronchomalacia
Pulmonary Edema in BPD • Reduced cross sectional area of pulmonary vessels causes increased pulmonary vascular resistance • Alveolar hypoxia induces local vasoconstriction • Intact vessels must accept remaining pulmonary blood flow, which leads to • elevated pressure and RV afterload • increased fluid filtration in interstitium
Clinical Course of BPD • Most: gradual improvement over weeks or months • Some: marked pulmonary instability in first few weeks followed by weeks or months of ventilator dependence • Few: pulmonary hypertension and cor pulmonale
Prevention of BPD • Antenatal glucocorticoid steroids - lead to decreased incidence RDS, but only modest decrease in BPD • Nutrition –although poor growth is associated with BPD, no studies show impact of nutrition in altering risk for BPD • Vitamin A – Slight decrease in BPD with IM supplementation in ELBW infants (Darlow, 2011), UW study showed increased sepsis with IM vit A (48.5% vs. 12%), but no decrease BPD • Surfactant – decreases risk of pneumothorax, improves survival, decreases need for oxygen and ventilation, but no decrease in rate of BPD.
Prevention of BPD (cont.) • Limited oxygen – SUPPORT trial with lower oxygen targets saw decreased incidence of ROP, but increased mortality and no decrease in BPD • Permissive hypercapnea – Target of pCO2>52 vs. <48 not associated with decreased BPD in ELBW, but decreased ventilation at 36 wks (Carlo, 2002) • HFOV – not associated with decreased BPD compared to modern conventional ventilation
Prevention of BPD (cont.) • PDA treatment – incidence of PDA goes up with ligation (Chorne, 2007) • Inhaled Nitric Oxide – NO-CLD trial showed decreased BPD in treatment group. Survival without BPD 43.9% vs. 36.8% (Ballard, 2006)
Ventilation Strategy for CLD Settings Slow Respiratory Rates < 40 breaths/min PIP (lowest required) target VT 5-10 mL/kg Not ECLS candidate PSV/VG PEEP 5-6 (up to 12 for bad TM) Short Inspiratory Times 0.4-0.7 s Blood Gases Permissive Hypercapnea pCO2 levels 45-65* pH 7.25-7.35 Less Aggressive Oxygenation Goals paO2 45-55* Saturations 85-92%
Management of established BPD:Bronchodilators • Beta-2 agonists (albuterol, terbutaline) acutely decrease airway resistance and increase compliance • Only one controlled clinical study of outcomes (Denjean, 1992) • 173 infants < 31 weeks, vent at 10 days • No effect on survival, severity of BPD, duration of vent or oxygen use
Management of established BPD:Bronchodilators • Recommendation (not evidenced-based!) • Use albuterol for short-term effects or to treat acute deterioration • Discontinue if no improvement in gas exchange, work of breathing, or number of respiratory decompensations • Watch for tachycardia, arrhythmia, hypokalemia, irritability
Management of established BPD:Acute Exacerbations • Consider viral infections (usually not bacterial) • Consider tracheitis if purulent secretions • Obtain CXR (although rarely helpful) • Culture and gram stain of tracheal secretions if purulent (often misleading) • Try dose of furosemide • Try inhaled albuterol, and if poor response, try ipratropium • Consider inhaled corticosteroids • Consider systemic corticosteroids for 5 days, esp. if at term corrected age
Web Resources for Parents • http://www.nhlbi.nih.gov/health/dci/Diseases/Bpd/Bpd_WhatIs.html • Excellent description of BPD for lay audience from the National Heart Lung and Blood Institute • http://www.nlm.nih.gov/medlineplus/ency/article/001088.htm • Very brief review of BPD from National Library of Medicine’s Medline Plus website • http://depts.washington.edu/growing/Assess/BPD.htm • Description of BPD with emphasis on home care and nutritional issues from Donna Johnson at the University of Washington