Download
1 / 75
760 likes | 949 Views
Uganda. Winnie Mwebesa, Save the Children John Stanback, Family Health International. Outline. Country Background Research on CBD of DMPA Scale-up in SC CBD program Scale-Up Research 2007-08 Policy on CBD Provision of DMPA Scale Up & Implementation Elsewhere in Uganda

E N D
Uganda Winnie Mwebesa, Save the Children John Stanback, Family Health International
Outline Country Background Research on CBD of DMPA Scale-up in SC CBD program Scale-Up Research 2007-08 Policy on CBD Provision of DMPA Scale Up & Implementation Elsewhere in Uganda Future Directions
Demographic Data Population: 30.7 million1 Rural Population: 87% 1 MMR: 435/100,000 live births U5MR: 138/1000 live births IMR: 76/1000 live births NMR: 32/1000 live births Total Fertility Rate: 6.71 Unmet Need for Family Planning: 40.6%1 ( Spacing: 24.5% - Limiting: 16.1%) CPR – modern contraception: 18% 1 Population Reference Bureau 2009 2 Uganda Demographic and Health Survey 2006
Contraceptive Prevalence(Modern Methods) STATCompiler – MEASURE Demographic and Health Surveys – UDHS 2006
Trends in fertility and FP use in Uganda Uganda DHS 1995 – 2000-2006
Socio-Economic Data Literacy2 Urban:84.9% Rural: 56.3% Religion2 Catholic: 42.4% Protestant: 34.5% Muslim: 11.2% GNI PPP Per Capita, 2007: 920 USD1 Out of pocket spending for health : 37% 3 1 Population Reference Bureau 2 Uganda Demographic and Health Survey 2006 3 Opportunity for Africa’s Newborns
Commitment to FP4 “The goal is to provide information and services that will enable individuals and couples to decide freely and responsibly when, how often and how many children to have. Objectives: Increase access to quality, affordable, acceptable and sustainable family planning services to everyone who needs contraception; Promote strong integrated family planning information and services in the health sector at all levels and within various ministries.” 4 - The National Policy Guidelines and Service Standards for Sexual and Reproductive Health and Rights
Health System Financing3 Per Capita Expenditure on Health Total: 25 USD Government: 7 USD General government expenditure on health (as a percentage of total expenditure on health): 26.9% General government expenditure on health (as a percentage of total government expenditure): 10.0% User protection fee for women and children exists 3 - WHO Statistical Information System
Structure of the Health System5 Services provided by public and private sector mix (private is more active in urban areas) Public structure is decentralized Districts receive block grants from the Ministry of Health (MoH) to deliver services Role of central MoH: technical support, supervision and monitoring, setting norms and standards, resource mobilization and donor coordination Government provides support to NGOs, but sector is primarily self-financed 5 – DFID, Uganda Country Health Briefing Paper 2000
Source of injectables Public sector : 36.2% Private sector: 62.1% DHS 2006
Main reasons for not using FP UDHS 2006
Save the Children CBD FP Program - Initially 3-year USAID funded project (2001 – 2004) Goal: improving access, quality and utilization of FP services in Nakasongola within 7 sub-counties 50 Community Health Reproductive Workers (CRHWS) provide information and services: free condoms, oral contraceptive pills, and referrals for DMPA Women’s preference for injectable contraception > 50% of women had to walk more than one mile to reach a health center
The Community Reproductive Health Worker package Volunteers selected by community to provide FP/RH services (free ) Coverage: number of households Training: Basic - 5 day (Community mapping, basic RH anatomy, contraceptive technology, FP counseling, Health education, record keeping and reporting) DMPA: initially 3 week – shortened to 10 day (1 week classroom – 1 week health center) Supervision: Health extension worker and Health Center II (reports – FP supplies – waste disposal) – monthly meetings – annual forum for experience sharing Incentives: equipment (gumboots, umbrella, bag); transport; bicycle; Challenges: attrition; maintaining motivation;
Pilot Study Key Results Nakasongola, Uganda, 2004-5 758 Depo acceptors followed to time of 2nd injection CBD vs. Clinic clients CBD results equal or better in: Safety Quality of care Continuation Satisfaction No infections or abscesses Source: Stanback J, Mbonye A, Bekiita M. “Contraceptive Injections by Community Health Workers in Uganda: A Non-Randomized Trial,” Bulletin of the World Health Organization, October 2007; 85:768–773
Injection Site Problems Pilot Study Results
Pilot Conclusion and Challenges Conclusion: With proper training and support, CBD provision of injectable contraception is safe, feasible, acceptable and improves access. Challenges: Sustainability of supplies (Depo and syringes) from government clinics Follow-up of CBD workers from Health Unit staff
Scale-up in SC CBD program Leveraged pilot study results 2006: secured funding from Flexible Fund and support from FHI Two additional districts in Central Uganda: Luwero & Nakaseke Total population: approximately 242,000 Mapped out existing CRHWs and trained additional Increasingly linking to VHT strategy
Scale-Up Research 2007-08 Scale-up vs. Pilot Outcomes Long term follow-up DMPA provision in rural drug shops
Scale-up versus Pilot Clients who received a 2nd Injection (6 mo. continuation)
Scale-up versus Pilot Clients who received a 2nd Injection (6 mo. continuation)
Scale-up versus Pilot Satisfaction with Care (“satisfied” or “very satisfied”) 95% 93%
Scale-up versus Pilot Satisfaction with Care (“satisfied” or “very satisfied”) 95% 93% 98%
Client Knowledge of Common Side Effects Scale-up versus Pilot
Client Knowledge of Common Side Effects Scale-up versus Pilot
Long Term Follow-Up of Original Cohorts Track down original CBD and clinic clients Assess recent FP and reproductive history
Drug Shop Operator Training Nursing or midwifery qualifications FP training 89% Infection prevention training Safe injection training
Drug Shop Operator Injection Safety Abscess prev. year Needle stick prev. year 14% Free access to sharps container Ever re-use syringes? 9%
Would you prefer getting Depo… From a clinic 34% From a CBD 22% Not sure 19% By self-injecting at home 24%
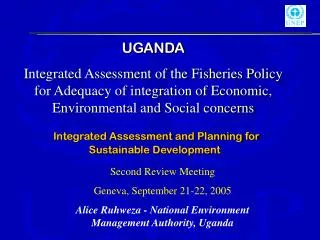
TUNISIA MOROCCO ALGERIA WESTERN LIBYA EGYPT SAHARA MAURITANIA MALI NIGER ERITREA SENEGAL SUDAN CHAD THE DJIBOUTI GAMBIA BURKINA FASO GUINEA GUINEA BISSAU BENIN NIGERIA TOGO ETHIOPIA SIERRA LEONE COTE D’VOIRE CENTRAL AFRICAN GHANA LIBERIA REPUBLIC CAMEROON SOMALIA DEMOCRATIC UGANDA KENYA EQUATORIAL REP. OF REPUBLIC GUINEA THE OF THE CONGO GABON CONGO RWANDA BURUNDI TANZANIA MALAWI ANGOLA ZAMBIA MOZAMBIQUE MADAGASCAR ZIMBABWE NAMIBIA BOTSWANA SWAZILAND LESOTHO SOUTH AFRICA Status of Paramedical Provision of DMPA in Africa 2009 National policies now permit and programs are planning for scale-up or scaling-up. Pilot or limited program implementation w/ MOH approval; national policy restrictions remain in place. Potential for introduction of a demonstration project and/or policy change.
Current Policy Permissive policy Uganda MOH national service guidelines do not support CHW provision of injectables