Download
1 / 30
310 likes | 337 Views
Learn about normal thyroid function, biosynthesis of thyroid hormones, and the mechanism of action of thyroid drugs. Discover important insights into absorption, metabolism, and hormonal balance.

E N D
Thyroid and Antithyroid Drugs Assist. Professor Dr. Hayder B Sahib PhD Pharmacology
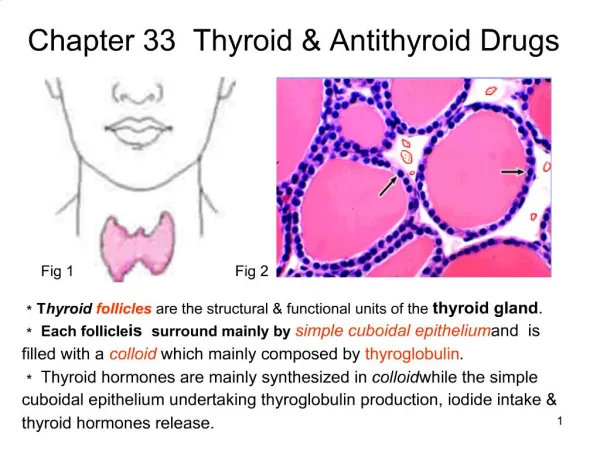
The normal thyroid gland secretes sufficient amounts of the thyroid hormones¾triiodothyronine (T3) and tetraiodothyronine (T4, thyroxine) • to normalize growth and development, body temperature, and energy levels. These hormones contain 59% and 65% (respectively) of iodine as an essential part of the molecule. • Calcitonin, the second type of thyroid hormone, is important in the regulation of calcium metabolism
Biosynthesis of Thyroid Hormones • Once taken up by the thyroid gland, iodide undergoes a series of enzymatic reactions that convert it into active thyroid hormone The first step is the transport of iodide into the thyroid gland by an intrinsic follicle cell basement membrane protein called the sodium/iodide symporter (NIS). This can be inhibited by such anions as thiocyanate (SCN-), pertechnetate (TcO4-), and perchlorate (ClO4-). • At the apical cell membrane a second I- transport enzyme called pendrin controls the flow of iodide across the membrane. Pendrin is also found in the cochlea of the inner ear and if deficient or absent, a syndrome of deafness and goiter, called Pendred's syndrome
At the apical cell membrane, iodide is oxidized by thyroidal peroxidase to iodine, in which form it rapidly iodinates tyrosine residues within the thyroglobulin molecule to form monoiodotyrosine (MIT) and diiodotyrosine (DIT). • This process is called iodide organification. • Thyroidal peroxidase is transiently blocked by high levels of intra-thyroidal iodide and blocked more persistently by thioamidedrugs.
Two molecules of DIT combine within the thyroglobulin molecule to form L-thyroxine (T4). One molecule of MIT and one molecule of DIT combine to form T3. • In addition to thyroglobulin, other proteins within the gland may be iodinated, but these iodoproteins do not have hormonal activity. • Thyroxine, T3, MIT, and DIT are released from thyroglobulin by exocytosis and proteolysis of thyroglobulin at the apical colloid border.
The MIT and DIT are deiodinated within the gland, and the iodine is reutilized. • This process of proteolysis is also blocked by high levels of intra-thyroidal iodide. • The ratio of T4 to T3 within thyroglobulin is approximately 5:1, so that most of the hormone released is thyroxine. • Most of the T3 circulating in the blood is derived from peripheral metabolism of thyroxine
The primary pathway for the peripheral metabolism of thyroxine is deiodination. • Deiodination of T4 producing 3,5,3¢-triiodothyronine (T3), which is three to four times more potent than T4. • Alternatively, deiodination may occur in the inner ring, producing 3,3¢,5¢-triiodothyronine (reverse T3, or rT3), which is metabolically inactive. • Drugs such as amiodarone, iodinated contrast media, B blockers, and corticosteroids, and severe illness or starvation inhibit the 5¢-deiodinase necessary for the conversion of T4 to T3, resulting in low T3 and high rT3 levels in the serum.
THYROID HORMONES • Thyroxine is absorbed best in the duodenum and ileum; absorption is modified by intraluminal factors such as food, drugs, and intestinal flora. • Oral bioavailability of current preparations of L-thyroxine averages 80% In contrast, T3 is almost completely absorbed (95%). • T4 and T3 absorption appears not to be affected by mild hypothyroidism but may be impaired in severe myxedema with ileus. These factors are important in switching from oral to parenteral therapy. • For parenteral use, the intravenous route is preferred for both hormones.
In patients with hyperthyroidism, the metabolic clearances of T4 and T3 are increased and the half-lives decreased; the opposite is true in patients with hypothyroidism. • Drugs that induce hepatic microsomal enzymes (eg, rifampin, phenobarbital, carbamazepine, phenytoin, imatinib, protease inhibitors) increase the metabolism of both T4 and T3 Despite this change in clearance, • the normal hormone concentration is maintained in euthyroid patients as a result of compensatory hyperfunction of the thyroid. However, patients receiving T4 replacement medication may require increased dosages to maintain clinical effectiveness.
A similar compensation occurs if binding sites are altered. • If TBG sites are increased by pregnancy, estrogens, or oral contraceptives, there is an initial shift of hormone from the free to the bound state and a decrease in its rate of elimination until the normal hormone concentration is restored. • Thus, the concentration of total and bound hormone will increase, but the concentration of free hormone and the steady-state elimination will remain normal. The reverse occurs when thyroid binding sites are decreased.
Mechanism of Action • the free forms of thyroid hormones, T4 and T3, dissociated from thyroid-binding proteins, entering the cell by active transport. • Within the cell, T4 is converted to T3 by 5¢-deiodinase, and the T3 enters the nucleus, where T3 binds to a specific T3 receptor protein, a member of the c-erb oncogene family. • The T3 receptor exists in two forms, a and b. Differing concentrations of receptor forms in different tissues may account for variations in T3 effect on different tissues. • Most of the effects of thyroid on metabolic processes appear to be mediated by activation of nuclear receptors that lead to increased formation of RNA and subsequent protein synthesis, eg, increased formation of Na+/K+ ATPase. This is consistent with the observation that the action of thyroid is manifested in vivo with a time lag of hours or days after its administration.
Large numbers of thyroid hormone receptors are found in the most hormone-responsive tissues (pituitary, liver, kidney, heart, skeletal muscle, lung, and intestine), while few receptor sites occur in hormone-unresponsive tissues (spleen, testes). • The brain, which lacks an anabolic response to T3, contains an intermediate number of receptors. • The number of nuclear receptors may be altered to preserve body homeostasis. • For example, starvation lowers both circulating T3 hormone and cellular T3 receptors.
Thyroid Preparations These preparations may be synthetic (levothyroxine, liothyronine, liotrix) or of animal origin (desiccated thyroid). • Synthetic levothyroxine is the preparation of choice for thyroid replacement and suppression therapy because of its • 1- stability • 2- content uniformity • 3- low cost • 4- lack of allergenic foreign protein • 5- easy laboratory measurement of serum levels • 6- long half-life (7 days), which permits once-daily administration. • In addition, T4 is converted to T3 intracellularly; thus, administration of T4 produces both hormones.
Although liothyronine (T3) is three to four times more potent than levothyroxine, it is not recommended for routine replacement therapy because of its • 1- shorter half-life (24 hours), which requires multiple daily doses • 2- its higher cost • 3- the greater difficulty of monitoring • 4- adequacy of replacement by conventional laboratory tests. • 5- its greater hormone activity and consequent greater risk of cardiotoxicity, • T3 should be avoided in patients with cardiac disease. It is best used for short-term suppression of TSH.
ANTITHYROID AGENTS • Thioamide • Thethioamidesmethimazole and propylthiouracil are major drugs for treatment of thyrotoxicosis. • carbimazole, which is converted to methimazolein vivo, is widely used. • Methimazole is about ten times more potent than propylthiouracil.
Pharmacokinetics • Propylthiouracil is rapidly absorbed, reaching peak serum levels after 1 hour. The bioavailability of 50-80% may be due to incomplete absorption or a large first-pass effect in the liver. • The volume of distribution approximates total body water with accumulation in the thyroid gland. • Most of an ingested dose of propylthiouracil is excreted by the kidney as the inactive glucuronide within 24 hours. • In contrast, methimazole is completely absorbed but at variable rates. • It is readily accumulated by the thyroid gland and has a volume of distribution similar to that of propylthiouracil. Excretion is slower than with propylthiouracil; 65-70% of a dose is recovered in the urine in 48 hours.
The short plasma half-life of these agents (1.5 hours for propylthiouracil and 6 hours for methimazole) has little influence on the duration of the antithyroid action or the dosing interval because both agents are accumulated by the thyroid gland. • Both thioamides cross the placental barrier and are concentrated by the fetal thyroid, so that caution must be employed when using these drugs in pregnancy. Because of the risk of fetal hypothyroidism, both thioamides are classified as pregnancy category D
propylthiouracil is preferable in pregnancy because it is more strongly protein-bound and, therefore, crosses the placenta less readily. • In addition, methimazole has been, rarely, associated with congenital malformations. • Both thioamides are secreted in low concentrations in breast milk but are considered safe for the nursing infant.
Pharmacodynamics • The thioamides act by multiple mechanisms. • The major action is to prevent hormone synthesis by inhibiting the thyroid peroxidase-catalyzed reactions and blocking iodine organification. • In addition, they block coupling of the iodotyrosines. • Propylthiouracil and (to a much lesser extent) methimazole inhibit the peripheral deiodination of T4 and T3 . • Since the synthesis rather than the release of hormones is affected, the onset of these agents is slow, often requiring 3-4 weeks before stores of T4 are depleted.
Toxicity • Adverse reactions to the thioamides occur in 3-12% of treated patients. Most reactions occur early, especially • 1- nausea and gastrointestinal distress. • 2- An altered sense of taste or smell may occur with methimazole. • 3- The most common adverse effect is a maculopapular pruritic rash (4-6%), at times accompanied by systemic signs such as fever. • Rare adverse effects include an urticarial rash, vasculitis, a lupus-like reaction, lymphadenopathy hypoprothrombinemia, exfoliative dermatitis, polyserositis, and acute arthralgia. Hepatitis (more common with propylthiouracil) and cholestatic jaundice (more common with methimazole) can be fatal; although asymptomatic elevations in transaminase levels also occur.
The most dangerous complication is agranulocytosis (granulocyte count < 500 cells/mm3), an infrequent but potentially fatal adverse reaction. • It occurs in 0.1-0.5% of patients taking thioamides, but the risk may be increased in older patients and in those receiving high-dose methimazole therapy (> 40 mg/d). The reaction is usually rapidly reversible when the drug is discontinued, but broad-spectrum antibiotic therapy may be necessary for complicating infections. • Colony-stimulating factors G-CSF; may hasten recovery of the granulocytes. • The cross-sensitivity between propylthiouracil and methimazole is about 50%;
Iodides • Prior to the introduction of the thioamides in the 1940s, iodides were the major antithyroid agents; today they are rarely used as sole therapy. • Pharmacodynamics • Iodides have several actions on the thyroid. • 1- They inhibit organification • 2- inhibit hormone release • 3- decrease the size and vascularity of the hyperplastic gland. In susceptible individuals, iodides can induce hyperthyroidism (jodbasedow phenomenon) or precipitate hypothyroidism. • In pharmacologic doses (> 6 mg/d), the major action of iodides is to inhibit hormone release, possibly through inhibition of thyroglobulin proteolysis.
Clinical Use of Iodide • Disadvantages of iodide therapy include an increase in intraglandular stores of iodine, which may delay onset of thioamide therapy or prevent use of radioactive iodine therapy for several weeks. • Thus, iodides should be initiated after onset of thioamide therapy and avoided if treatment with radioactive iodine seems likely. • Iodide should not be used alone, because the gland will escape from the iodide block in 2-8 weeks, and its withdrawal may produce severe exacerbation of thyrotoxicosis in an iodine-enriched gland. • Chronic use of iodides in pregnancy should be avoided, since they cross the placenta and can cause fetalgoiter. • In radiation emergencies, the thyroid-blocking effects of potassium iodide can protect the gland from subsequent damage if administered before radiation exposure.
Toxicity • Adverse reactions to iodine (iodism) are uncommon and in most cases reversible upon discontinuance. They include • 1- acneiform rash (similar to that of bromism), • 2-swollen salivary glands, • 3-mucous membrane ulcerations, • 4-conjunctivitis, • 5-rhinorrhea, • 6- drug fever, metallic taste, • 7-bleeding disorders and, rarely, anaphylactoid reactions.
4. Iodinated Contrast Media • The iodinated contrast agents¾diatrizoate orally and iohexol orally or i.v¾are valuable in the treatment of hyperthyroidism, although they are not labeled for this indication. • These drugs rapidly inhibit the conversion of T4 to T3 in the liver, kidney, pituitary gland, and brain, a decrease in heart rate is seen after only 3 days of administration of 0.5-1 g/d of oral contrast media. • T3 levels often return to normal during this time. The prolonged effect of suppressing T4 as well as T3 suggests that inhibition of hormone release due to the iodine released may be an additional mechanism of action.
Fortunately, these agents are relatively nontoxic. They provide useful adjunctive therapy in the treatment of thyroid storm and offer valuable alternatives when iodides or thioamides are contraindicated. • Surprisingly, these agents may not interfere with 131I retention as much as iodides despite their large iodine content. • Their toxicity is similar to that of the iodides, and their safety in pregnancy is undocumented.
5. Radioactive Iodine • 131I is the only isotope used for treatment of thyrotoxicosis . Administered orally in solution as sodium 131I, it is rapidly absorbed, concentrated by the thyroid, and incorporated into storage follicles. • Its therapeutic effect depends on emission of B rays with an effective half-life of 5 days Within a few weeks after administration, destruction of the thyroid parenchyma is evidenced by epithelial swelling and necrosis, follicular disruption, edema, and leukocyte infiltration. Advantages of radioiodine include easy administration, effectiveness, low expense, and absence of pain. Radioactive iodine should not be administered to pregnant women or nursing mothers, since it crosses the placenta to destroy the fetal thyroid gland and is excreted in breast milk.
6. Adrenoceptor-Blocking Agents • Beta blockers without intrinsic sympathomimetic activity (eg, metoprolol, propranolol, atenolol) are effective therapeutic adjuncts in the management of thyrotoxicosis since many of these symptoms mimic those associated with sympathetic stimulation. • Propranolol has been the b blocker most widely studied and used in the therapy of thyrotoxicosis. Beta blockers cause clinical improvement of hyperthyroid symptoms but do not alter thyroid hormone levels.