Download
1 / 20
200 likes | 417 Views
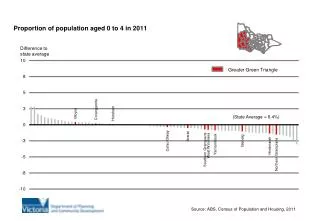
Developing a Chronic Disease Model of Care for Coronary Artery Disease and Depression in Rural Settings. Dr Steve Bunker Prof James Dunbar Dr Prasuna Reddy Greater Green Triangle University Department of Rural Health. The Greater Green Triangle Region. Why depression?.

E N D
Developing a Chronic Disease Model of Care for Coronary Artery Disease and Depression in Rural Settings Dr Steve Bunker Prof James Dunbar Dr Prasuna Reddy Greater Green Triangle University Department of Rural Health
In 2003, the National Heart Foundation of Australia (NHFA) published the results of an evidence-based review which concluded that depression is an independent predictor for adverse cardiac outcomes. (Bunker S. et al. Med J Aust 2003;178:272-6) These findings have since been incorporated by the NHFA into clinical practice guidelines for preventing cardiovascular events in people with coronary heart disease. (Reducing Risk in Heart Disease. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand, 2004. Background
Depression and relative risk of developing CHD Age HT Stage 2 Smoking Diabetes LDL>160 HDL<35 Depressed Mood ClinicalDepression 0 1 2 3 4 5 Low Risk High Risk
Depression following myocardial infarction Survival free of cardiacmortality, cumulative % Days after MI Discharge
The INTERHEART Study Yusuf, S., et al. The Lancet 3rd Sept 2004
Musselman, D. et al. (1998). The Relationship of Depression to Cardiovascular Disease. Epidemiology, Biology and Treatment. Archives of General Psychiatry 55: 580-592.
Cardiovascular will remain the leading cause of disease burden The ten leading causes of disease burden in developed countries 1990–2020 2020 disease or injury2 1990 disease or injury1 Rank order Ischaemic heart disease Ischaemic heart disease 1 Cerebrovascular disease Cerebrovascular disease 2 Unipolar depression Road traffic accidents 3 Trachea bronchus & lung cancers Trachea bronchus & lung cancers 4 Road traffic accidents Self-inflicted injuries 5 Alcohol use Perinatal conditions 6 Osteoarthritis Lower respiratory infections 7 Dementia and other CNS disorders Congenital anomalies 8 Chronic obstructive pulmonary disease Colon and rectal cancers 9 Self-inflicted Injuries Stomach cancer 10 1. Murray and Lopez. Global Burden of Disease Study. 1996. 2. Murray and Lopez. Global Burden of Disease Study. 1997 Note: Disease burden is measured in disability-adjusted life years (DALYs), a measure that combines the impact on health of years lost due to premature death and years lived with a disability. One DALY is equivalent to one lost year of healthy life
The aim of this study, funded by the National Heart Foundation of Australia, is to implement the evidence-based guidelines into routine clinical practice. A model of care, incorporating a clinical pathway, will be developed to identify depressive symptoms in acute coronary syndrome (ACS) patients at the time of hospital discharge and eight weeks later when assessed in the primary care setting. Aim
Identification of current activities in Australia and overseas in relation to the development and implementation of clinical pathways for depression and CHD and other co-morbid chronic illness. Gaining management commitment from participating organisations. Creating a Clinical Pathways Team, scoping the Pathway and developing Process Maps. Health Provider Interviews. Discovery Interviews with patients and carers at discharge and 8 weeks. Interviews with GPs of patients at 8 weeks. Identifying best practice model of care for specific patient groups. Pilot implementation of model of care and evaluation of guidelines. Methodology
South Australia: Mount Gambier Hospital Limestone Coast Division of General Practice Victoria: Wimmera Health Care Group West Vic Division of General Practice Target Numbers 30 patients (+ carers, GPs) in Mount Gambier 30 patients (+ carers, GPs) in Wimmera Study Sites
Steps Admission interview with patient and carer Interviews with health staff Eight week interview with patient and carer GP interview at eight weeks Process mapping day Process Mapping the Patient Journey
57 patients (22 Women & 35 Men) 57 carers (mainly spouses and adult children) 18 Health Professionals 18 General Practitioners Participants
Continuity of care (not just a tool to pick up) Ask them specific questions (including family history) Rating scale tool (must be concise as there is not time) Political issues: not enough funding for rural mental health Public awareness, education Time is a problem (may need to tell the receptionist to get a longer consultation) GP suggestions to identify acute coronary syndrome patients with psychological issues such as depression
Depression is hard to identify by interview Symptomsseldom volunteered by patient Patients, carers and health care providers generally attribute the symptoms of depression to the heart disease itself Rate of identified depression well below rates reported from studies of hospitalised patients using routine screening Conclusions
When should patients be screened? (a) Prior to discharge (b) 8 weeks from the event and (c) 3 to 6 months from the event What screening tool should be used? HADS and PHQ 9 Who should do the screening? (a) Cardiac rehab nurse (b) GP or Practice nurse Where should patients be screened? (a) Hospital (b) Cardiac rehab (c) Primary care Previous history of depression needs to be assessed Recommendations
Evidence-based best practice model of care for people with co-morbid depression and coronary heart disease: Pilot implementation plan for Mt Gambier and District Health Service and Limestone Coast Division of General Practice (Hawkins Medical Centre) Pilot Implementation
Chronic Disease Management: Depression and CHD NHFA Guideline Practice Protocol
Proposed intervention (modified from Rozanski*) Stepped Interventions Degree Of Psychosocial Distress Examples Add mental health care specialist, and nurse manager Step 3 SEVERE Add BOMH, nurse manager, and adherence promotion (eg telephone follow-up) Step 2 MODERATE GP and nurse follow up Step 1 MILD *Rozanski, et al. Psychosocial Risk Factors in Cardiac Practice. J Am Coll Cardiol 2005;45:637–51