Download
1 / 26
280 likes | 472 Views
Surgery and hypertension . Presented by: Dr. Rana Chowdhury . . What is HYPERTENSION Hypertension is defined as a rise in blood pressure over and above the normal range for the age of a patient for three consecutive setting.

E N D
Surgery and hypertension. Presented by: Dr. Rana Chowdhury.
What is HYPERTENSION Hypertension is defined as a rise in blood pressure over and above the normal range for the age of a patient for three consecutive setting. In normal healthy subject, normal range of systolic blood pressure is 110 to 140 mm Hg and that of diastolic pressure is 60 to 90 mm of Hg.
Incidence: Hypertension is one of the most common chronic medical conditions worldwide. The incidence of hypertension increases with age and affects men at a slightly higher rate than women. Considering the prevalence of chronic hypertension, the management of patients with chronic hypertension undergoing surgery is of major clinical importance as these patients are at an increased risk of morbidity and mortality during or after surgery.
Hypertension in surgical patient • High blood pressure is discovered during routine physical examination for a surgical disorder. • Patient on medical treatment for essential hypertension may develop a surgical condition that requires treatment. • Surgical treatment is required for a disorder causing secondary hypertension.
Importance of hypertension in surgical patient: The importance of hypertension in a surgical patient mainly relates to the fact that the hypertensive patient is at a higher risk of having coronary artery disease. Patients with preoperative hypertension are known to be more likely to show exaggerated fluctuations in blood pressure during surgery, often associated with ECG evidence of myocardial ischemia.
These blood pressure fluctuations could be important, since intraoperative myocardial ischemia correlates with post operative cardiac morbidity. It follows, therefore, that, control of blood pressure preoperatively should help to reduce the tendency to blood pressure fluctuations during surgery and to perioperative myocardial ischemia. This is the rationale behind ensuring that the resting BP is controlled prior to surgery.
Clinical assessment of preoperative hypertension: It is desirable that the hypertensive patient undergoes full clinical assessment prior to surgery. This should focus on three issues. • First, careful review of whether existing medications are controlling the blood pressure and when necessary, additional therapy is instituted.
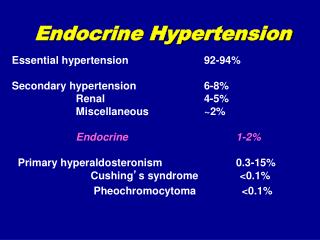
Second, whether the hypertension has produce any target organ damage, specially, with regard to checking the ECG changes in LVH and renal function. Any target organ damage increases the operative risks. • Third, to exclude rare secondary causes of hypertension, the principle one being phaeochromocytoma, that could lead to enormous problems during surgery if it was not diagnosed before-hand.
Other clues as to secondary causes of hypertension are hypokalaemia which would alert the surgeon to the possibility of Conn’s syndrome, a radial to femoral artery delay, indiacative of coarctation and an abdominal bruit which might suggest renal artery stenosis.
Perioperative risks and their management • In hypertensive patients, induction of anaesthesia is often associated with large reductions in arterial pressure. This may precipitate myocardial ischaemia as the diastolic pressure falls thus reducing both the coronary and the cerebral perfusion pressures. In these circumstances vasopressors may be indicated.
Laryngoscopy and intubation often cause large increases in blood pressure. Protection can be obtained with β-blockers including labetalol and i.v. bolus doses of esmolol. Glyceryltrinitrate, sodium nitroprusside, prostaglandin E1 and fentanyl have all been shown to be effective as well as deep anaesthesia, droperidol, and administration of vasodilators such as hydralazine and calcium channel blockers. As hypertension associated with tachycardia can cause myocardial ischaemia, prevention of the hypertensive response to laryngoscopy, intubation, and extubation is advisable.
Severe perioperative hypertension is a major threat to hypertensive patients, especially increases of blood pressure in excess of about 20% of the preoperative value. Consequences of pressure surges include bleeding from vascular suture lines, cerebrovascularhaemorrhage, and myocardial ischaemia/infarction. The mortality rate of such events may be as high as 50%.
Perioperative hypertensive crises are generally caused by a sympathetically mediated increase in peripheral vascular resistance. The choice of the most appropriate antihypertensive therapy depends upon the clinical scenario, i.e. whether there is tachycardia, myocardial ischaemia, cardiac failure, or renal functional impairment
Preoperative Management of hypertension Anti hypertensive medication should be continued throughout the perioperative period in order to maintain control of blood pressure and prevent rebound hypertension. In particular patients, beta blocker therapy should not be withdrawn even if this requires the use of parenteral beta blockers in patient unable to take oral medication.
If blood pressure needs to be controlled more before surgery, then, some manipulation of the patient’s oral therapy can normally be undertaken with a successful result in a few days and hence, surgery does not need to be delayed unduly. If surgery is required more urgently, rapidly acting agents specially beta blockers can be used to control blood pressure in a few minutes or hours.
Antihypertensive therapy is now known to reduce the incidence of complications, such as, Myocardial Infarction, Cerebrovascular accident, Heart failure and Renal failure. The four classes of drugs commonly used are: • Thiazide diuretics, • Beta blockers, • Ca Antagonists, • ACE inhibitors. • A new class of drug, called the Angiotensin-II receptor antagonists is now being used more widely for the treatment of essential hypertension.
There is an interesting paradox here in that, patients with preoperative hypertension are more likely to develop intraoperative hypotension than patients who were normotensive preoperatively. This intraoperative hypotension can be associated with perioperative cardiac events. Although intraoperative hypotension can be a problem in hypertensive patient, this is not a reason for relaxing blood pressure control preoperatively.
Specially since the intraoperative hypotension may be a consequence of intraoperative ischemia rather than the primary event.
Summary: The hypertensive patient requires careful pre operative assessment to make sure that blood pressure is controlled and to exclude secondary causes. These may require surgery to be delayed somewhat, but hypertension itself seldom causes anything more than a slight delay to surgery.
Refference: • Essential Surgical Practice – A. Cuschieri. • Short practice of Surgery - Bailey & Love. • Current Surgical Diagnosis & Treatment – Gerard M. Doherty. • The surgical hypertensive patient - P Foëx,DPhil FRCA FMedSci, Emeritus Nuffield Professor of Anaesthetics, Nuffield Department of Anaesthetics, The John Radcliffe Hospital, Headley Way, Oxford, PhD FRCA. • Perioperative management of hypertension - Norman M Kaplan, MD • Perioperative hypertension management - Joseph Varon and Paul E Marik.