Download
1 / 16
220 likes | 538 Views
UTI in Children. NICE Guidelines Mary Conroy. Common condition May present with non specific symptoms Sequelae, heavy burden on NHS. Diagnosis < 3 months. Fever Vomiting Lethargy Poor feeding/FTT Abdominal pain /jaundice/haematuria/offensive urine. Preverbal Fever Abdominal/loin pain

E N D
UTI in Children NICE Guidelines Mary Conroy
Common condition • May present with non specific symptoms • Sequelae, heavy burden on NHS
Diagnosis < 3 months • Fever • Vomiting • Lethargy • Poor feeding/FTT • Abdominal pain /jaundice/haematuria/offensive urine
Preverbal Fever Abdominal/loin pain Vomiting Lethargy FTT Haematuria Offensive urine Verbal Frequency Dysuria Dysfunctional voiding Changes to continence Pain Cloudy/offensive urine Diagnosis > 3 months
When to test urine • with symptoms and signs of UTI • with unexplained fever of 38°C or higher (test urine after 24 hours at the latest). • with an alternative site of infection but who remain unwell (consider urine test after 24 hours at the latest).
Collecting the urine sample • A clean catch urine sample is the recommended method for urine collection. • – use other non-invasive methods such as urine collection pads. • – do not use cotton wool balls, gauze or sanitary towels. • If other non-invasive methods are not possible: • – use a catheter sample or suprapubic aspiration • Do not delay treatment if the sample cannot be obtained and the infant or child is unwell
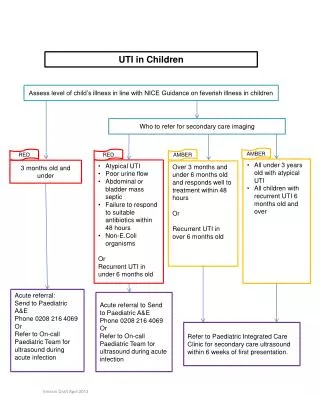
Under 3/12 0 refer to paeds • 3/12 – 3 years – urgent miscroscopy and culture + Abx or MC&S + Abx
Management • Under 3/12 refer • Upper UTI/Pyelonepritis, consider referral Cef or Augmentin 7-10 days • Lower UTI, oral antibiotics 3 days eg trimethoprim, nitrifurantoin, amoxicillin
Prevention • Hydration • Try not to delay voiding • Address dysfunctional elimination syndromes and constipation
Investigation < 6/12 • Typical UTI (responds to Tx 48hr) - US within 6 weeks • Atypical UTI/ Recurrent UTI - US during acute infection, DMSA, MCUG
6/12 – 3 years • Typical UTI – nil • Atypical UTI – US during acute infection DMSA • Recurrent – US DMSA
Over 3 years • Typical UTI – Nil • Atypical UTI – US acute • Recurrent UTI – US DMSA
Follow up • Refer recurrent UTI and abnormal imaging • Renal parenchymal defects – monitor height, weight, BP and proteinuria • Long term follow up: bilateral renal abnormalities, impaired renal function, BP, proteinuria under paeds nephrologist to slow progression to CKD
Summary • Consider UTI in the febrile child • Refer <3/12, consider in upper UTI/Atypical UTI • Typical UTI > 6/12 – no need for investigation