Download
1 / 15
150 likes | 390 Views
Diagnosis & Management of UTI in Children – May 2005. Dr N Ali – Paediatric SHO. Facilitated by: The Clinical Governance & Effectiveness Department . Objectives To ensure prompt diagnosis and treatment of UTI in children while keeping diagnostic tests to a minimum.

E N D
Diagnosis & Management of UTI in Children – May 2005 Dr N Ali – Paediatric SHO Facilitated by: The Clinical Governance & Effectiveness Department
Objectives • To ensure prompt diagnosis and treatment of UTI in children while keeping diagnostic tests to a minimum. • To assess the degree of compliance to the standards and protocols at JPH.
Rationale • UTI is one of the most common bacterial infections in childhood, accounting for up to 5% of febrile illnesses. • Diagnosis may be missed in infants and young children due to non specific nature of their symptoms. • Significant risk that UTI will give rise to: • Serious acute illness • Permanent renal damage
Methodology Part 1-Diagnosis • Retrospective study of 20 patients in the time period of Feb 05 identified from ward 10 register. Part 2-Managment • Retrospective audit • Children < 5 years admitted or referred to JPH with proven UTI. • Duration of audit July 2004-Dec 2004 • Random collection of 39 children were identified.
Management of UTI - sample size The patients’ D numbers were taken from the Laboratory; which included Ward 10, A&E attendees and GP referrals. • Total number of patients for the Management of UTI is 39. (<1 year = 11 >1 year = 28). • Number of patients included in audit: 19 (<1 year = 9 >1 year = 10). • A&E attendees / GP referrals (excluded from audit): 20 (<1 year = 2 >1 year = 18).
A&E attendees / GP referrals For patients with proven UTI 100 (18/18) 100 (2/2)
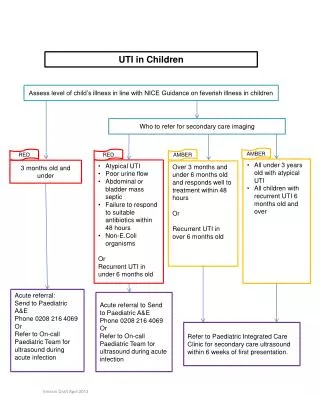
Diagnosis of UTI – Criterion 1 Urine will be tested in any infant with a temperature above 38.5°C and will be sent to the lab if positive for nitrates and / or leucocytes. (No exceptions) 45% 55% (9/20) (11/20) (n=20)
Management of UTI – Criterion 2 Children under the age of 1 year with proven UTI will have: • An ultrasound examination of the kidneys and bladder (No exceptions) • MCUG (No exceptions) • DMSA (No exceptions) • Urgent ultrasound, if applicable (Exc: Not applicable) 78 (7/9) 100 (9/9) % 67 56 (6/9) (5/9) 22 (2/9) 33 44 (3/9) (4/9) 0 (0/9) (n=9)
Management of UTI – Criterion 3 Children over the age of 1 year with proven UTI will have: • An ultrasound examination of the kidneys and bladder (No exceptions) • DMSA, if applicable (Exc: Not applicable) • MCUG, if applicable (Exc: Not applicable) 70 (7/10) 90 (9/10) 70 (7/10) % 30 (3/10) 20 (2/10) 0 (0/10) 10 10 (1/10) (1/10) (n=10)
Management of UTI – Criterion 4 Children will have Plain Abdominal X-ray taken, if applicable. (Exc: Not applicable) 11% (2/19) 89% (17/19) (n=19)
Management of UTI – Criterion 5 Children <1 year of age OR with recurrent UTI will start prophylaxis in accordance with guidelines when treatment for UTI completed. (No exceptions) 22% (2/9) 78% (7/9) (n=9)
Additional Information 02 What was the cause of infection? (n=39) • E. Coli: 58% (23/39) • Proteus: 8% (3/39) • Coliform: 23% (9/39) • Debris: 5% (2/39) • Mixed bacterial growth: 3% (1/39) • No growth: 3% (1/39)
Additional Information 03 Were there any pre-disposing factors? Other includes; Kidney problems, antenatal left renal pelvic dilatation, enlarged right kidney and antenatally detected hydronephrosis.
Conclusions • Higher proportions of children at GP practice with proven UTI were not referred to JPH for further management. • Urine dipstick is not routinely tested or documented in children with febrile illness or other presentations. • MSU results not acted upon in few cases especially in children < 1 year therefore were missed for further management.
Recommendations • Strict adherence to the guidelines. • Paediatricians and GP’s should work together to establish local policies on method of treatment and follow up of patients not admitted to hospital. • Urine dipstick should be done and documented. • To check urine culture results as soon as available and agreed plan of action. • To re-audit to monitor performance and demonstrate improvement on current practice.