Download
1 / 20
210 likes | 419 Views
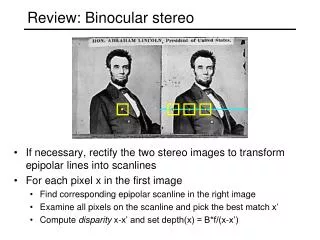
BINOCULAR DYSFUNCTION REMEDIATION II. VERGENCE THERAPY. Vergence Dysfunctions . Run along the horizontal axis of the new fangled, BVA ‘O’ MATIC CHART Less severe: towards center More severe: towards periphery. AE. PCE 2ºAE. LOW/ NORMAL. HIGH/ NORMAL. CE. CI. LOW. HIGH. HIGH/

E N D
BINOCULAR DYSFUNCTION REMEDIATION II VERGENCETHERAPY
Vergence Dysfunctions • Run along the horizontal axis of the new fangled, BVA ‘O’ MATIC CHART • Less severe: towards center • More severe: towards periphery
AE PCE 2ºAE LOW/ NORMAL HIGH/ NORMAL CE CI LOW HIGH HIGH/ NORMAL LOW/ NORMAL PCI PCE 2ºAI AI
Vergence Dysfunctions • Off horizontal axis: increased accommodative involvement • Lower: • Left: PCI • Right: PCE (2º accommodative insufficiency) • Upper: PCE (2º to accommodative excess)
AE PCE 2ºAE LOW/ NORMAL HIGH/ NORMAL CE CI LOW HIGH HIGH/ NORMAL LOW/ NORMAL PCI PCE 2ºAI AI
Convergence Insufficiency • More severe at left edge • Anti-suppression and accommodation are secondary modalities to address • 3-4 vergence/1-2 anti-suppression activities first 1-3 sessions • Incorporate 2 accommodative activities after 4th session
Convergence Excess • More severe at right edge • Usually expect smaller “gains” each week of Tx compared with insufficiency • Accommodation is a secondary modality to address • 5 vergence activities first 2-3sessions • Incorporate 2 accommodative activities after 3rd session
Pseudo CI’s • Spread out, away from the horizontal axis • Bottom left: “Classic” Pseudo CI • Usually requires 2.5 activities of Accomm. and vergence throughout Tx! • Closely monitor for A/S problems • Takes longer to remediate than other vergence Dx
Pseudo CE Secondary to Accommodative Insufficiency • Spread out, away from the horizontal axis • Bottom right: Pseudo CE 2º AI • Usually requires an initial add • may be enough to remediate problem • 3 accommodative activities /2 vergence activities
Pseudo CE Secondary to Accommodative Excess • Spread out, away from the horizontal axis • Top right: Pseudo CE 2º AE • Accommodative excess is usually the most dramatic feature here • Rarely above 2-3 prism diopters esophoria at near • Accommodative facility (relaxation) significantly affected • 3 accommodative activities/2 vergence expected
General Approach for Vergence Dysfunction: • “Rock” a patient from something they can accomplish with ease to something difficult • This mantra of BV is still applied at the end of therapy (i.e. begin integrated convergence work with minus and BI).
General Approach for Vergence Dysfunction: Vergence Starting Point • Vergence activities usually begun at the transitional level • At times, very basic “walk-towards/away” therapy is necessary for several sessions
General Approach for Vergence Dysfunction: Accommodative Technique Starting Point • A vergence patient with normal skills: • Will have difficulty controlling and adjusting vergence output with binocular level techniques • Would not be able to maintain vergence at a steady state on binocular accommmodative rock • In many cases, only 2-3 sessions at the trasitional level for vergence skills is required.
General Approach for Vergence Dysfunction: Anti-Suppression Starting Point • Necessary if your therapy grinds to a halt because of suppression • May occur at either the transitional or binocular level, for any modality.
General Approach for Vergence Dysfunction: Anti-Suppression Starting Point • Blinking, flashing a penlight at the suppressing eye or tapping the target being suppressed may be all that is required • When suppression is still preventing progress, the following activities would be called for:
Anti-Suppression Activities • Transitional: • Vis-a-vis • Red/red rock without dioptric lenses • Doell’s Mazes or Litetrac series • Brock BU series/Morgenstern Basic Fusion cards • Binocular: • Cheiroscopic tracings • AN and EC series
General Approach for Vergence Dysfunction: Oculomotor Starting Point • Oculomotility skills may be affected in children with vergence dysfunction. • A relatively high correlation exists between true convergence insufficiency and oculomotor dysfunction. • When necessary, one (out of 5) activity in the orthoptics session will be OM
Cases: True CI (case #............) • Vergence dysfunction • Bad combination of • Low AC/A ration • Insufficient compensating vergence ranges (BO) • DDx from Psuedo CI includes: • Difficulty w/+ on binocular accomm. Facility • No trouble w/ monocular • No plus acceptance/low lag/lead of accommodation
Cases: Pseudo CI (case #..........) • Accommodation dysfunction w/ vergence “side-effects” • Bad combination of • Poor accommodative control • debilitated vergence ranges (BO) “gives up the nearpoint ship”
Cases: Pseudo CI (case #..........) Cont. • DDx from true CI includes: • Difficulty clearing MINUS on monocular and binocular +/-2.00 facility • May have difficulty with plus binoc. facility (if PRC is low enough) • Plus acceptance/high lag • some improvement with plus