Download
1 / 10
140 likes | 434 Views
Liver Injuries. Liver - # 2 most commonly injured organ in blunt abdominal trauma Right Lobe >>> Left Lobe Posterior segment > anterior segment Caudate injury is rare, usually in assoc w/ right or left lobe injury Mortality blunt traumatic hepatic trauma – 8-25% (uncontrolled hemorrhage).

E N D
Liver Injuries • Liver - # 2 most commonly injured organ in blunt abdominal trauma • Right Lobe >>> Left Lobe • Posterior segment > anterior segment • Caudate injury is rare, usually in assoc w/ right or left lobe injury • Mortality blunt traumatic hepatic trauma – 8-25% (uncontrolled hemorrhage)
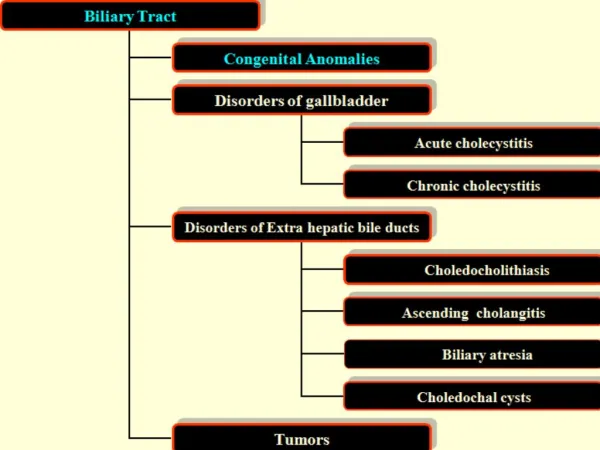
Liver Injury Forms • Laceration • Intrparenchymal hematoma • Infarction • Subcapsular hematoma
American Association of Trauma Surgery – Hepatic Injury Scale • I – Capsular tear, < 1 cm parenchymal depth • II – Parenchymal tear, 1-3 cm depth • III – Parenchymal disruption, > 3cm depth but involving < 25% of the hepatic lobe • IV – Parenchymal disruption, 25-50% of hepatic lobe • V – Parenchymal disruption - > 50% of hepatic lobe • VI – Hepatic avulsion
Driver of pick up truck rear-ended by another truck @ 40mph Hemodynamically stable – BP 140’s/70’s, HR 80’s Abdomen – soft, nondistended, tender w/ voluntary guarding Also with open LE fx Hct 4334 during hospital course ALT 599, Alk phos 73, LA 1.7 CT Abd/pelvis done Grade IV Liver laceration V-shaped – occupies entire 4a segment Intact hilum Subcapsular hematoma Free fluid in pelvis No active extravasation Management – SICU observation, no transfusions, HD stable, 5 days bed rest, on floor, plan to d/c to home 22 yr female
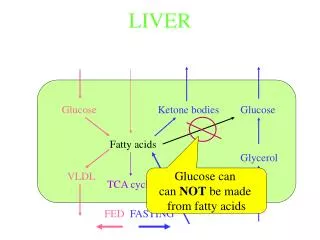
Management Options • Non-operative management of blunt hepatic and splenic injuries = TOC in HD stable pts, irrespective of injury grade • No evidence for routine imaging of HD stable, clinically improving pt • HD unstable = surgery vs. selective hepatic artery embolization (portal system supplies flow to de-arterialized tissue until collaterals develop)
References • Practice Management Guidelines for the Nonoperative Management of Blunt Injury to the Liver and Spleen, 2003 Eastern Association for the Surgery of Trauma • Nonoperative management of blunt hepatic trauma: The exception or the rule?, Journal Trauma 1994. Jason Zolak CC IV