Download

1 / 13
130 likes | 187 Views
UK Radiotherapy Trials QA (RTTAQ) Group. SBRT trial QA programmes. GHG meeting - ESTRO May 2017. QA Programme: NHSE CtE (England only) (NHS England Commissioning through Evaluation). UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy.

E N D
UK Radiotherapy Trials QA (RTTAQ) Group SBRT trial QA programmes GHG meeting - ESTRO May 2017
QA Programme: NHSE CtE (England only)(NHS England Commissioning through Evaluation)
UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy Collaborative work: Trialists, RTTQA and UK SABR consortium Adopted by the NHSE CtE and in clinical use for current and future SABR trials Submitted for publication: UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy Hanna GG, Patel R, Aitken A, et al UK stereotactic Ablative Radiotherapy trials normal tissue dose constraints tolerance consensus. 2016; Radiother. Oncol. 119:1; S191
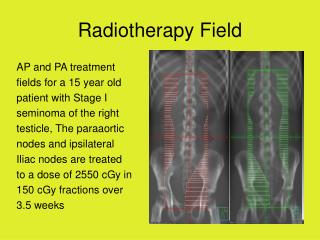
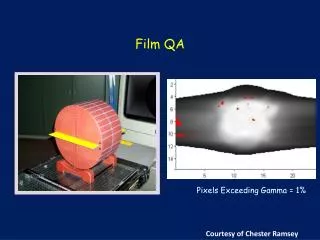
Lung audit • 37centres audited • As required for trial /commissioning programme • Single machine, single energy • Motion management not assessed • Postal audit using CIRS Model 002LFC IMRT thorax phantom • EBT3 GafChromic film - planar dosimetry • Alanine dosimeters – dose at target volume centre • CT dataset of phantom with pre-defined volumes (ITV) sent to centres for planning • Alanine results showed planned and delivered doses were within ±3.0% for 34/37 SABR plans
Spinal audit • SABR Spine dosimetry audit • CIRS E2E SBRT phantom • Dosimetry • Axial GafChromic Film (yellow) • Alanine and MicroDiamond detectors (orange) • Measurement in bone CTV (red) and water equivalent cord
Outlining benchmark • Same cases for all centres • Reviewed against a standard by study CI +/- TMG members • Drop down menus: • No variation (per-protocol) • Acceptable (variation) • Unacceptable (variation)
Planning benchmark • Same cases for all centres • Reviewed against protocol prescription and mandatory and optimal dose constraints by RTTQA
Individual case review • Prospective: • Turnaround time 48-72hrs • Outlines submitted for review prior to plan • Amendments to outlines and plan implemented and re-reviewed before treatment • Pressure to avoid delays to planned treatment start date • Report format same as benchmark case review • Retrospective: • Timely retrospective - within first week of treatment • Standard retrospective - during trial • No direct feedback to centres
What has worked …and what hasn’t! • Audit logistics • Borrowing phantoms • Coordination of audit aspects from multiple centres • Audit limitation • Non standard local plan, harder to provide feedback • No movement • Workload • Many treatment sites • Underestimated number of clinicians • Huge workload for individual centres and RTTQA • Planning aspects more challenging with higher failure rate compared to outlining • Lung case relatively easy as well established. • Liver case hardest to set up – motion management issues. Liver contouring high failure rate. • Audit cost and familiarity (borrowing local phantoms) • Consistency of treatment across all centres • Streamlining - faster trial QA approval • Positive feedback from majority of centres • Enabled inexperienced centres to clinically implement SABR with support • Learning experience for centres with similar equipment • Large data set • An overall view of what is achievable with specific equipment combinations • Facilitate future development of plan metrics