Download
1 / 17
180 likes | 236 Views
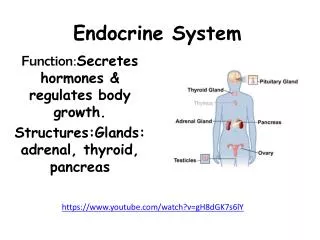
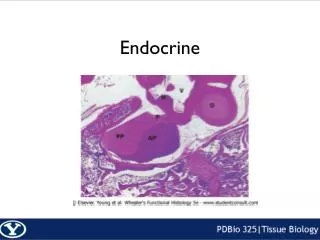
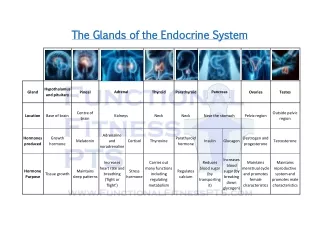
ENDOCRINE. ENDOCRINE PANCREAS. Diabetes Mellitus. Blood glucose values are normally maintained in a very narrow range, usually 70 to 120 mg/dL. The diagnosis of diabetes is established by noting elevation of blood glucose by any one of three criteria:

E N D
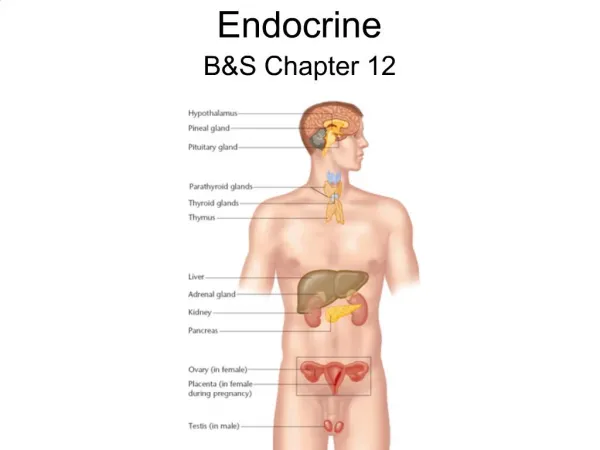
ENDOCRINE PANCREAS
Diabetes Mellitus • Blood glucose values are normally maintained in a very narrow range, usually 70 to 120 mg/dL. The diagnosis of diabetes is established by noting elevation of blood glucose by any one of three criteria: • A random glucose > 200 mg/dL, with classical signs and symptoms • A fasting glucose > 126 mg/dL on more than one occasion • An abnormal oral glucose tolerance test (OGTT), in which the glucose is > 200 mg/dL 2 hours after a standard carbohydrate load
Hormone production in pancreatic islet cells.Immunoperoxidase staining shows a dark reaction product for insulin in β cells (A), glucagon in α cells (B), and somatostatin in δ cells (C).D, Electron micrograph of a β cell shows the characteristic membrane-bound granules, each containing a dense, often rectangular core and distinct halo.
CLASSIFICATION • Type 1 diabetes is characterized by an absolute deficiency of insulin caused by pancreatic β-cell destruction. It accounts for approximately 10% of all cases. • Type 2 diabetes is caused by a combination of peripheral resistance to insulin action and an inadequate secretory response by the pancreatic β-cells ("relative insulin deficiency"). Approximately 80% to 90% of patients have type 2 diabetes.
MORPHOLOGY OF DIABETES AND ITS LATE COMPLICATIONS Pancreas. • Reduction in the number and size of islets • Leukocytic infiltration of the islets • β-cell degranulation • In type 2 diabetes, there may be a subtle reduction in islet cell mass • Amyloid replacement of islets in type 2 diabetes
A, Insulitis, shown here from a rat model of autoimmune diabetes, also seen in type 1 human diabetes. B, Amyloidosis of a pancreatic islet in type 2 diabetes.
Diabetic Nephropathy • The kidneys are prime targets of diabetes. Renal failure is second only to myocardial infarction as a cause of death from this disease. • Three lesions are encountered: • (1) glomerular lesions; • (2) renal vascular lesions, principally arteriolosclerosis; • (3) pyelonephritis, including necrotizing papillitis. • The most important glomerular lesions are capillary basement membrane thickening, diffuse mesangial sclerosis, and nodular glomerulosclerosis.
Severe renal hyaline arteriolosclerosis Note a markedly thickened, tortuous afferent arteriole. The amorphous nature of the thickened vascular wall is evident.
Renal cortex showing thickening of tubular basement membranes in a diabetic patient (PAS stain).
Electron micrograph of a renal glomerulus showing markedly thickened glomerular basement membrane (B) in a diabetic. L, glomerular capillary lumen; U, urinary space.
Nephrosclerosis in a patient with long-standing diabetes. The kidney has been bisected to demonstrate both diffuse granular transformation of the surface (left) and marked thinning of the cortical tissue (right). Additional features include some irregular depressions, the result of pyelonephritis, and an incidental cortical cyst (far right).
INFECTIONS in Dm • SKIN • TUBERCULOSIS • PNEUMONIA • PYELONEPHRITIS • CANDIDA
NEOPLASMS of the Endocrine Pancreas • Islet cell tumors • Beta cells INSULINOMAS (NOT rare) • Alpha cells GLUCAGONOMAS (rare) • Delta cells SOMATOSTATINOMAS (rare) • GASTRINOMAS, producing ZOLLINGER-ELLISON SYNDROME, consisting of increased acid and ulcers