Download

1 / 79
800 likes | 1.07k Views
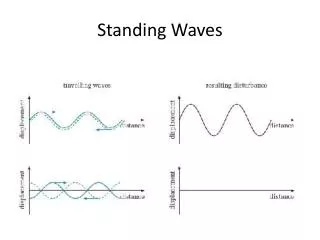
Standing Field Treatment Protocols (SFTPs). Los Angeles County EMS Agency. Phase One Introduction Question/Answer SFTPs/Teaching Points Introduction To Scenarios. Phase Two General Review Question/Answer Scenarios - Discussion. SFTP Training Schedule. Phase One. Introduction.

E N D
Standing Field Treatment Protocols(SFTPs) Los Angeles County EMS Agency
Phase One Introduction Question/Answer SFTPs/Teaching Points Introduction To Scenarios Phase Two General Review Question/Answer Scenarios - Discussion SFTP Training Schedule
Phase One Introduction
SFTP Training Program Goals • To Prepare Paramedics To Utilize SFTPs In Situations Where They Are Appropriate And To Recognize Situations Where Base Hospital Contact Is Required Or Recommended. • To Develop Understanding Of Treatment Protocols And Apply Them Utilizing Structured Scenarios.
SFTP Training Program Objectives • At The Completion Of This Training Program, Participants Will Be Able To: • Understand the reasons for implementation of SFTPs • Identify information that must be reported to hospitals receiving protocol patients • Discuss the issue resolution process for SFTPs • Discuss appropriate interventions for each protocol
SFTP Training Program Objectives • Identify situations where base hospital contact is required when SFTPs are utilized • Verbalize understanding of perfusion parameters • Verbalize understanding of SFTP application using structured scenarios
SFTP Introduction • Set Of Algorithms • Expedite And Improve Field Care By Eliminating The Need For Base Contact On Some (Not All) Common Chief Complaints • Based On Presenting Signs/Symptoms And Chief Complaint • Based On Existing Los Angeles County Base Hospital Treatment Guidelines
General Considerations • Reference No. 806, Procedures Prior To Base Contact • Protocols May Be Combined • Documentation • Transport When Appropriate • Saline Locks When Appropriate • Perfusion • Basics (Airway, O2, Reassessment)
Question #1Why SFTPs? • Standardization Of Treatment • Expedite Patient Care • Reduce Time Spent On Communications
Question #2Provider Agencies Utilizing SFTPs • Los Angeles Fire Department (April 1997) • Culver City Fire Department (January 1998) • Burbank Fire Department (October 1998) • Long Beach Fire Department (April 1999) • Alhambra Fire Department (April 1999) • San Marino Fire Department (June 1999) • West Covina Fire Department (Feb. 2000) • Los Angeles County Sheriff Dept. (May 2005) • Santa Monica Fire Department (January 2006) • Downey Fire Department (August 2008)
Question #3Paramedic SFTP Prerequisites • At Least One Member Of Each Two Paramedic Team Must have A Minimum Of One Year Experience As A Paramedic and Both Must be Accredited in LA County • Both Must Have Completed SFTP Training • Staffing Exceptions • Combining Resources
Question #4Paramedic Responsibilities • Fundamental Change In Prehospital Care • Increased Autonomy • Greater Accountability • Complete Patient Assessment • Accurate Documentation
M2 (ALOC) M4 (Chest Pain) M7 (Abd. Pain) M9 (OD) M17 (Respiratory Distress) – Covers SOB, Rales , Wheezing M13 (Adult Seizure) M14 (Neuro. Deficit) M15 (Syncope) CA (Cardiac Arrest) Question #5Medical Chief Complaints Covered Under SFTPs
P1 (Active Labor) P2 (Newborn) P5 (Pediatric Seizures) Question #5 OB/Pediatric Chief Complaints Covered Under SFTPs
T1 (Burns) T2 (Minor Trauma) T3 (Major Trauma) T4 (Trauma Arrest)) Question #5Trauma Chief Complaints Covered Under SFTPs
Symptomatic Dysrhythmias Poor Perfusion (Medical Patients) Environmental Allergic Reaction Anaphylaxis Dystonic Reaction Neonatal Resuscitation Pediatric Arrest Question #6Chief Complaints NOT Covered Under SFTPs
Question #7 Base Hospital Contact • Base Contact As Usual When Chief Complaint Is Not Covered Under SFTPs • Base Contact Is Required When: • Unlisted Treatments May Be Necessary • Signs And Symptoms Are Complex Or Not Clearly Encompassed In The Protocol • Paramedics Desire Consultation With The Base Hospital
Question #8Base Contact After A Protocol Has Been Initiated • Medical Patients Being Treated By A Protocol, May Initially Appear Stable And Then Exhibit Signs Of Poor Perfusion • Base Contact Is Required Regardless Of What Point Is Reached In The Protocol
Question #9Additional Information • When The Base Hospital Requests Additional Information - Give The Information • Address Issues After The Run With The Individual, The PCC And/Or The Paramedic Coordinator
Question #10Second Opinion • Base Contact Should Be Made When The Paramedic Feels Uncomfortable For Any Reason Or Has A Question About An Aspect Of Patient Care • If Protocol Treatment Has Been Initiated - Give The Base A Full Report And Describe The Treatment(s) Rendered Prior To Contact
Question #11Hospital Diversions • Each Provider Agency Has A Specific Plan For Identifying Hospitals On Diversion • Current Mechanisms: • Agreement With Base Hospital • Agreement With Receiving Hospital • ReddiNet In Dispatch • ReddiNet In Each Rig
Question #12Hospital Notification • Each Provider Agency Has A Specific Plan: • Current Mechanisms: • Base Hospital Contact • Direct Call To Receiving Hospital By Cellular Telephone
Question #12 SFTP Notification - Medical Patient • Provider Code/Unit # • “We Have A Protocol Patient” • Sequence Number (if calling Base Hospital) • Age/Gender of the Patient • Name of the Protocol(s) (Number Optional) • Level of Distress • Destination/ETA • If STEMI Patient, Notify Base of Such
Question #12SFTP Notification - Minor Trauma • Provider Code/Unit # • “We Have A Minor Trauma Protocol Patient” • Age/Gender Of The Patient • Mechanism Of Injury • Level Of Distress • Location of Injury • Destination/ETA
Provider Code/Unit # “We have a Major Trauma Protocol Patient by ------” Sequence Number Age/Gender MOI Level of Distress Location of Injuries Complete Vital Signs GCS Airway Adjuncts Utilized Pertinent Information Destination/ETA Question #12SFTP Notification - Major Trauma
Questions #13 Trauma Center Patients • Must Go To Trauma Center For: • Trauma Criteria • Trauma Guidelines • Paramedic Judgement • In Most Cases Paramedics Will Contact Trauma Center Directly • Trauma Patients That Do NOT Meet Trauma Criteria/Guidelines May Be Treated Under the Minor Trauma Protocol
Question #14AMAs • Base Contact Required For Patients Meeting 808.1 Section I Criteria • Documentation MUST Be Complete (High Risk Incidents)
Question #15Transfer Of Care To A Non-SFTP Provider • Base Contact Required • Advise The Base Hospital That Patient Care Is Being Transferred to A Non-SFTP Provider
Question #16Transport Of SFTP Patient With One Paramedic And One EMT-I • Provided That Two Qualified Paramedics Are On Scene - SFTPs May Be Utilized • If The Patient Condition Deteriorates During Transport - Base Contact Is Required
Question #17Paramedic Interns Assigned To An SFTP Provider • Inform Intern That SFTPs May Only Be Utilized By Approved SFTP Providers • Interns Are Not Evaluated On Their Knowledge Of SFTPs • Allow Paramedic Interns To Perform Radio Communication Skills
Question #18SFTP Quality Improvement • Provider Agency • Outcome Data From Base and Receiving Hospitals • EMS Agency Review
Phase One SFTPs/Teaching Points
Introduction To The Protocols • Simple Format • Based On Existing Los Angeles County Base Hospital Treatment Guidelines • Must Be Followed As Written • Patient Reassessment After Each Medication Or Treatment And Throughout The Call • Pediatric Dosages Are Indicated By A “Teddy Bear” Symbol
Base Contact Required • Medical Patients With Signs Of Poor Perfusion • Symptomatic Dysrhythmias • Chief Complaints That Are Not On A Protocol • Deviations From The Protocol • When Specified By The Protocol • Consultation In Complex Cases
Determination of Perfusion • Hypotension • Tachydysrhythmias/Bradydysrhythmias • Shortness Of Breath • Skin Signs/Capillary Refill • Chest Pain • Shortness Of Breath
General ALS • Medical Patients With Vague Complaints Who Do Not Require Medications Or Fluids • Basic And Advanced Airway Management • Cardiac Monitor If Indicated • Precautionary IV (PRN) • Blood Glucose Test (PRN) • When Would Base Contact Be Required?
M2 (ALOC) • Use The Appropriate Protocol If: • Overdose (M9) • Seizure (M13) • Acute Neurological Deficit (M14) • Blood Glucose Testing - Correct Procedure • Dextrose 50% Or Glucagon If No IV Access • Consider Narcan If Suspicious Of Narcotic OD, Treat By Overdose (M9) Protocol • When Would Base Contact Be Required?
M4 (Chest Pain) • Suspected Cardiac Related Pain (> 30 yrs.) • Steps 1 - 8 • Suspected Cardiac Related Pain (<30 yrs) • Contact base hospital for medication orders • Suspected Non-cardiac Pain (All Ages) • Steps 1 - 4 only(no medications) • When Would Base Contact Be Required?
Nitroglycerin Hold BP <100 systolic Shock Position If Hypotension Develops May Administer Prior To Venous Access Do NOT Include NTG Taken Prior To EMS Sexually Enhancing Drug precautions Reassess Vital Signs Aspirin Used For Anticoagulant Effect (not pain relief) Give Even If Patient: Has Taken Their Own ASA Is On Anticoagulants Contraindications: GI Bleeding Ulcer Disease ASA Allergy M4 (Chest Pain) - continued
M4 (Chest Pain) - continued • Morphine • Hold if BP < 100 Systolic • ONLY Given After 3 Doses Of NTG Are Documented To Be Ineffective • Observe Respiratory Status
M7 (Nontraumatic Abdominal Pain) • Use For Perfusing Patients With Nontraumatic Abdominal Pain • Cardiac Pain May Present As Abdominal Pain - Consider Using M4 (Chest Pain) Protocol • Basic Airway/Oxygen • Cardiac Monitor Prn/Document Rhythm • Venous Access Prn • Consider Treating Pain With Morphine
M9 (Overdose/Poisoning) • Protect Airway/Cardiac Monitor • Consider Blood Glucose • Narcan Administration: IV, IM. • Used to increase the rate and depth of respiration • When Would Base Contact Be Required?
M13 (Seizures - Adult) • Use For Witnessed Or Suspected Seizures • If BLS Transport Is Appropriate And No ALS Interventions Are Performed, Not M13 • Appropriate Airway Management • Midazolam 2-5mg slow IVP For Active Tonic/Clonic Seizures (maximum dose 10mg) • Blood Glucose • When Is Base Contact Required? • When Would A Trauma Center Be Considered?
M14 (Stroke) • Document Neurological Assessment (mLAPSS) • Document Symptom Onset Time • Glucose Test Required • Hyperventilation ONLY If Rapid Deterioration • When Is Base Contact Required?
M15 (Syncope) • If Patient Remains ALOC Use M2 Protocol • If Signs Of Poor Perfusion Persist - Base Contact Is Required • Blood Glucose Test Prn • Cardiac Monitoring Is Required To Rule Out Dysrhythmia • When Would Base Contact Be Required?
M17 (Respiratory Distress) Used In The Treatment Of: • Diminished/Absent Breath Sounds • Wheezing • Rales • Goal Is To Improve Ventilation And Oxygenation • When Would Base Contact Be Required?
M17 (Respiratory Distress- Rales) • Consider Non-cardiac Causes For Rales (Pneumonia Is The Most Common) • Wheezing May Be The Only Sign Initially – Albuterol via HHN or Hand Held Mask May Be Administered • CPAP, For Those Agencies Approved For It’s Use, Should Be Considered Early on In The Treatment Regime • Monitor Cardiovascular Status Carefully! • When Should Base Contact Be Considered? • When Would Base Contact Be Required?
M17 – (Rales Continued) • Nitroglycerin • Aggressive NTG Therapy Is Utilized To Reduce Preload And Afterload • Systolic BP > 100 = 0.4mg (1 puff) • Systolic BP > 150 = 0.8mg (2 puffs) • Systolic BP > 200 = 1.2mg (3 puffs) • Hold if BP < 100 systolic/patient on Viagra • If Hypotension Develops - Elevate Legs
Albuterol Hand Held Nebulizer or Hand Held Mask Consider Cardiovascular Effects Reevaluate Lung Sounds & Pulse Oximetry Frequently CPAP – Consider In Severe Cases – Decreases the Work Of Breathing – Can Minimize The Need For Intubation – Currently Not For Use With Pediatric Patients (< 14 years) Epinephrine Patients Under 40 Years Not in Pregnancy Used If Deteriorating Respiratory Status M17 (Respiratory Distress - Wheezing)






![General Protocols Of Hyperbaric Oxygen Treatment [HBOT]](https://cdn4.slideserve.com/7369871/general-protocols-of-hyperbaric-oxygen-treatment-hbot-dt.jpg)