Download

1 / 15
160 likes | 318 Views
Evasion and submersion of immune responses. Tuberculosis. Tuberculosis showed that the disease most often caused by Mycobacterium tuberculosis, but sometimes caused by M.bovis or M.africanum Tuberculosis is spread through contaminated air by the bacterium M. tuberculosis

E N D
Tuberculosis Tuberculosis showed that the disease most often caused by Mycobacterium tuberculosis, but sometimes caused by M.bovis or M.africanumTuberculosis is spread through contaminated air by the bacterium M. tuberculosis bacteria can survive in air for several hours Fetus can be infected from their mothers before or during the delivery process by inhaling or swallowing of contaminated amniotic fluid Babies can be infected by inhaling air containing the bacteria In developing countries, children infected by other micobacterium that causes tuberculosis M. bovis, which can be spread through milk is not sterilized
Immune evasion stratefies adapted by M. Tuberculosis • Some bacteria that are engulfed by macrophages have evolved means of avoiding destruction by these phagocytes and instead use macrophages as their primary host cell • After uptake by macrophages M. tuberculosisarrests phagosome maturation at the stage of an early endosome • Mycobacterium tuberculosis, for example, is taken up by macrophages but prevents the fusion of the phagosome with the lysosome, protecting itself from the bactericidal actions of the lysosomal contents • Many bactericidal pathways of macrophages are disrupted by M. Tuberculosis infection involves: killing by O2 and N2 radicals killing by acidification of phagosome Destruction by acid hydolases of phagosome • Further adaptations include the preventing macrophage cell death by inducing cell survival pathways • Escape recognition by T cells by down regulating MHC II
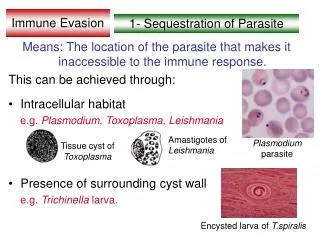
Evasion of macrophage mediated killing • Listeria and shigellaare the species which escape phagosome before its destruction • survives inside the vacuole until nutrients exhaust and then the cell bursts to spread infection • Legionella- can form a protective vacuole by secreting ER and golgi proteins onitsmemrane rather than the endocytic markers
Listeriamonocytogenes- pathogenesis • Listeriamonocytogenesis a Gram-positive rod-shaped bacterium • It is the agent of listeriosis, a rare but serious infection caused by eating food contaminated with the bacteria • Listeriosis has been recognized as an important public health problem in the United States • The disease affects primarily pregnant women, newborns, and adults with weakened immune systems • Listeriosis is a serious disease for humans; the overt form of the disease has a mortality greater than 25 percent • The two main clinical manifestations are sepsis and meningitis • Meningitis is often complicated by encephalitis (brain inflamation), a pathology that is unusual for bacterial infections Microscopically, Listeria species appear as small, Gram-positive rods, which are sometimes arranged in short chains
Listeriamonocytogenes- immune evasion • Listeriamonocytogenes, escape from the phagosome into the cytoplasm of the macrophage, where they multiply • They colonize non-professional APCs such as hepatocytes and enterocytesin order to escape the immune surveillance due to the low antigen presentation potential • The question is that how do they gain entry into these cells? • By expressing surface ligands such as internalin which binds to E- cadherin normally expressed by the cells to form tight junctions to the next cell (enterocytes) leading to internalization of the bacterium • They then spread to adjacent cells in the tissue without emerging into the extracellular environment • They do this by hijacking the cytoskeletal protein actin, which assembles into filaments at the rear of the bacterium • The actin filaments drive the bacteria forward into vacuolar projections to adjacent cells; the vacuoles are then lysed by the Listeria, releasing the bacteria into the cytoplasm of the adjacent cell • In this way Listeriaavoids attack by antibodies, but the infected cells are still susceptible to killing by cytotoxic T cells
Mycobacterium leprae • Mycobacterium lepraehas a difficult time replicating outside of host cells • Leprosy is characterized by bacterial replication inside intracellular vesicles of macrophages, Schwann cells, and endothelial cells • In general, M. leprae prefers such cells at lower temperatures than that of the human body, which is why it tends to manifest itself near the skin’s surface • The bacteria gains entry into the cells through receptor- mediated internalization process • Usually, after phagocytosis, bacteria are killed through fusion with a phagolysosome and digestion by proteases and oxidizing chemicals • However, M. leprae is somehow able to arrest the lysosome fusion process for anywhere from 1 to 4 hours and replicate inside the phagosome
Two types of Mycobacterium leprae infection • Cell mediated immunity is extremely important during the infection process of M. leprae due to the inability of B-cells to mount a useful immune response to pathogen • T-cell and macrophage responses to Mycobacterium /leprae are sharply different in the two polar forms of leprosy. • tuberculoid leprosy (a milder form of leprosy) • In lepromatousleprosy • In tuberculoid leprosy , growth of the organism is well controlled by T H 1-like cells (IL-2, IFN-y, and TNFa) that activate infected macrophages • IFN-y would be expected to activate macrophages, enhancing the killing of M. Leprae • The tuberculoid lesion contains granulomas and is inflamed, but the inflammation is local and causes only local effects, such as peripheral nerve damage • In lepromatous leprosy infection is widely disseminated and the bacilli grow uncontrolled in macrophages; • in the late stages of disease there is major damage to connective tissues and to the peripheral nervous system • Cytokines typically produced by TH2 cells (IL-4, IL-5, and IL-10) dominate in the lepromatousform
In tuberculoid leprosy, in contrast, there is strong cell-mediated immunity with macrophage activation that controls, but does not eradicate, infection • In lepromatous leprosy, cell-mediated immunity is profoundly depressed, cells infected with Mycobacterium leprae are present in great profusion, and cellular immune responses to many other antigens are suppressed
tuberculoid leprosy (a milder form of leprosy) • lepromatous leprosy
Immune evasion strategies by some bacteria • Suppression of antibodies: • Two notable bacteria that suppress the bodies reaction against them are Mycobacterium leprae- leprosy, and Mycobacterium tuberculosis, - tuberculosis • In both cases, the Interleukin-2 response to the bacteria is reduced. • In lepromatous leprosy, it has been shown that suppressor T cells, taken from the skin lesions caused by the disease, inhibit the responses of other T cells to Mycobacterium leprae antigens • Mycobacterium leprae : can also invade and inhabit cells that are not a part of the immune system, e.g. skin cells • Killing the Phagocyte: • Some bacteria are capable of releasing toxins that are lethal to Phagocytes. So instead of the invading bacteria being destroyed, the defending phagocytes are themselves destroyed • Among the bacteria that are capable of this strategy are Mycobacterium tuberculosis, Streptococcus pyogenes, some Staphylococci, and Bacillus Anthracis (the bacterium that causes the disease Anthrax) • Colonising the Phagocyte: • This highly successful strategy involves the invading bacteria allowing themselves to be Phagocytosed, but resisting being killed once they are inside the Phagocyte • Many types of bacteria use Macrophages as sites of sanctuary, where they can multiply without interference from other cells of the immune system. As mentioned above, bacteria that use this strategy include Mycobacterium leprae and Mycobacterium tuberculosis
spirochaetes- Introduction • Spirochetes are simple bacteria, with less than 1000 genes • Each type has a characteristic helical shape • Some are tightly coiled like a telephone cord, while others are more open • Very tight coils are seen in Leptospira, medium coils in Treponema and open coils are seen in Borrelia. • Spirochetes are Gram-negative and with a flagellar bundle running through their periplasmic space • The spirochete flagella run in the perplasmic space, causing the cells to move in a corkscrew fashion
Treponemapallidum- syphilis • The spirochete bacterium Treponemapallidum- the cause of syphilis • Syphilis is spread mostly by sexual contact, except for congenital syphilis, which is spread from mother to fetus • Transmission by sexual contact requires exposure to moist lesions of skin or mucous membranes • The symptoms of syphilis occur in three stages called primary, secondary and late: • The first sign of syphilis is a lesion known as a "chancre" (a clean, painless, indurated ulcer) which forms at the site of entry where the organism enters the body through the mucous membranes or breaks in the epithelium • Multiple chancres occur if more than one organism enters • Common sites for the lesions include genitalia, rectum, urethra and mouth. • The chancre, which may be accompanied by swollen glands, may last from one to five weeks, and may disappear by itself even if no treatment is received. • Approximately six weeks after the sore first appears, the second stage of the disease begins • The most common symptom during this stage is a rash, which may appear on any part of the body • Other symptoms may occur such as tiredness, fever, sore throat, headaches, hoarseness, loss of appetite, hair loss and swollen glands. • These signs and symptoms will last two to six weeks and generally disappear in the absence of adequate treatment
The third stage, called late syphilis (syphilis of over four years' duration), may involve illness in the skin, bones, central nervous system and heart. Untreated, syphilis can lead to destruction of soft tissue and bone, heart failure, blindness and a variety of other conditions which may be mild to incapacitating • Women with untreated syphilis may transmit the disease to unborn children, which can result in death or deformity of the child • Syphilis remains infectious for a period of up to two years, possibly longer. • Transmission of infection depends on the existence of infectious lesions (sores), which may or may not be visible • No natural immunity to syphilis develops and past infection offers no protection to future exposure • Syphilis is relatively easily treated with antibiotics such as penicillin, usually given as consecutive daily intramuscular injections • Patients who are allergic to penicillin may be treated with tetracycline
Immune evasion by Spirochaetes • The spirochete bacterium Treponemapallidum, the cause of syphilis, can avoid elimination by antibodies and establish a persistent and extremely damaging infection in tissues • T. pallidumis believed to avoid recognition by antibodies by coating its surface with host proteins until it has invaded tissues such as the central nervous system, where it is less accessible to antibodies • Another spirochete, the tick-borne Borreliaburgdorferi, is the cause of Lyme disease, which occurs as a result of chronic infection by the bacterium • Some strains of B. burgdorferimay avoid lysis by complement by coating themselves in the complement-inhibitory protein factor H made by the host which binds to receptor proteins in the bacterium's outer membrane