Download

1 / 28
290 likes | 611 Views
Toxicity of Targeted Therapy Christoph Zielinski Clinical Division of Oncology Department of Medicine I Medical University Vienna Central European Cooperative Oncology Group www.meduniwien.ac.at/krebszentrum www.cecog.org. Impact of Anti-EGFR Therapy. Chemotherapy refractory tumors

E N D
Toxicity of Targeted TherapyChristoph ZielinskiClinical Division of OncologyDepartment of Medicine IMedical University ViennaCentral European Cooperative Oncology Groupwww.meduniwien.ac.at/krebszentrumwww.cecog.org
Impact of Anti-EGFR Therapy • Chemotherapy refractory tumors • BOND study: Monotherapy vs. Combined Therapy • Front-line therapy in CRC Combination with FOLFIRI or FOLFOX • improved RR/PFS/OS ? • CORE Study (CECOG): FOLFOX + Cetuximab vs. FOLFIRI + Cetuximab • CRYSTAL study: FOLFIRI vs FOLFIRI + Erbitux • Neoadjuvant Therapy in Nonresectable Liver Metastases ... • Adjuvant Therapy in CRC and NSCLC • FOLFOX-4 +/- Erbitux in CRC • Maintenance Therapy after Chemotherapy Induction... • Additive / Synergistic Potential of Trastuzumab and Cetuximab in HER-2/neu 1+ / 2+ Overexpressing Breast Cancer…? • CECOG Phase I Study Testing for Radiosensitizing Activity in Rectal and Pancreatic Cancers • Radiosensitizing Activity in SCCHN • First- and Second-Line Treatment of SCCHN
BOND-Trial Efficacy Results: Response to Treatment. [ ] = 95% CI D. Cunningham et al., N Engl J Med 2004;351:337-345.
BOND Study: Time to ProgressionTotal Population Group Irinotecan + Erbitux 1 Erbitux N 218 111 No. events 92 152 0.8 Median 1.5 4.1 0.6 HR: 0.54 [95% CI: 0.42; 0.71]Log Rank p-Value < 0.0001 Proportion 0.4 0.2 0 0 2 4 6 8 10 12 Months D. Cunningham et al., N Engl J Med 2004;351:337-345.
BOND Study: Overall SurvivalTotal Population Group Irinotecan + Erbitux 1 Erbitux N 111 218 No. events 75 140 0.8 Median 6.9 8.6 HR: 0.91 [95% CI: 0.68; 1.21]Log Rank p-Value = 0.48 0.6 Proportion 0.4 0.2 0 0 2 4 6 8 10 12 14 16 Months D. Cunningham et al., N Engl J Med 2004;351:337-345.
Correlation of Response Rate and EGFR Expression Combination n/N (%) Monotherapy n/N (%) % EGFR-Expressing Cells 10 25/109 (22.9) 4/56 (7.1) > 10 - 20 4/20 (20.0) 5/16 (31.3) > 20 - 35 6/27 (22.2) 0/7 (0.0) >35 15/62 (24.2) 3/32 (9.4) EGFR-Staining Intensity faint 11/53 (20.8) 1/21 (4.8) weak/moderate 22/89 (24.7) 7/55 (12.7) strong 17/75 (22.7) 4/34 (11.8)
Erbitux Skin Toxicity • 80% incidence • Acne like rash • Xerosis, Paronychia, Lashes • Responds to Antibiotics • Resolves with Interruption • Grade of Acne-Like Rash may Correlate with Response Rate Photographs courtesy of Dr Siegfried Segaert and used with permission
The BOND Study:Grade 3/4 Toxicities (NCI-CTC v2.0) D. Cunningham et al., N Engl J Med 2004;351:337-345.
Cetuximab + FOLFOX-4 in mCRC: Grade 3/4 Adverse Events NCI CTC v2.0 No grade 3/4 Hypersensitivity / Allergic Reactions Observed Tabernero J et al. Proc Am Soc Clin Oncol 2004; abstract #3512, 2004
IFL + Cetuximab in mCRC:Selected Grade 3/4 Toxicities. NCI CTC v2.0 Rosenberg et al. Proc Am Soc Clin Oncol 2002; Abstract #536.
LUCAS Study in NSCLC: Overall Survival 1.00 Cetuximab/CTXCTX 12 m 32% 26% 18 m 14% 0 24 m 14% 0 Survival Distribution Function 0.75 0.50 0.25 0.00 0 5 10 15 20 25 Overall Survival (months) Rosell et al. Proc Am Soc Clin Oncol 2004; Abstract 7012
Cetuximab + CT (%) CT (%) Neutropenia Grade 4 21 (50%) 4 (10%) 16 (37%) 4 (10%) Nausea/vomiting 7 (17%) 6 (14%) Asthenia/fatigue 8 (19%) 1 (2%) Infection 2 (5%) 1 (2%) Fever/chills/sweating 4 (10%) 2 (5%) Thrombocytopenia 2 (5%) 1 (2%) Acne-like rash 2 (5%) 0 Diarrhoea 1 (2%) 0 Hypersensitivity reaction 1 (2%) 0 LUCAS Study: Grade 3/4 Toxicities per Patient for Multiple Cycles.NCI-CTC v2.0 Rosell et al. Proc Am Soc Clin Oncol 2004; Abstract 7012
Cetuximab/CT Group (n=43) CR+PR /All % • Skin Toxicities • None • Any • Grade 1 • Grade 2 • Grade 3 2 / 8 25% 37% 13 / 35 4 / 17 24% 4 / 13 31% 100% 5 / 5 LUCAS Study: Subset Analysis. Rosell et al. Proc Am Soc Clin Oncol 2004; Abstract 7012
Presence and Intensity of Rash Predicts Increased Survival. 14 12 10 Survival (months) 8 6 4 2 0 CRC CRC CRC CRC Pancreatic SCCHN Study: 9923 0141 BOND EORTC/NCI Saltz (2001)1 Saltz (2004)2 Cunningham Van Cutsem Abbruzzese (2001)5 Kies (2002)6 (2004)3 (2004)4 No reaction Grade 1 Grade 2 Grade 3 1. Saltz et al. Proc Am Soc Clin Oncol 2001;19: Abstract #7. 2. Saltz et al. J Clin Oncol 2004;22:1201-1208. 3. Cunningham D…Van Cutsem E. N Engl J Med 2004;351:337-345. 4. Van Cutsem et al. EORTC/NCI Geneva 2004. 5. Abbruzzese et al. Proc Am Soc Clin Oncol 2001; Abstract #518; 5. Kies et al. Proc Am Soc Clin Oncol 2002;20: Abstract #925.
Sub-Group Analysis: Correlation of Skin Reaction and Efficacy. Erbitux + irinotecan (N=218) • Skin reactions appear to be predictive for efficacy • Reactions can be effectively managed
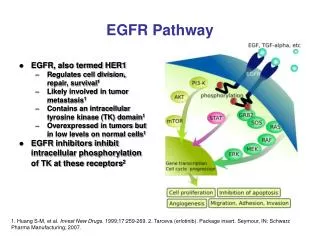
Current and Future Challenges Lynch. N Engl J Med 2004. • Prediction of Response Selection of Patients • Efficacy (Over)-Expression of the Target • Predictive markers • pEGFR • pMAPK • AKT, STAT3 • EGFR Gene Mutations Leading to Altered Sensitivity to TKIs1 • “Skin Rash Test”: Dose Escalation until Response? Translational Research Needed
Treatment Considerations • Most effective dose • Most effective regimen • Most effective schedule EVEREST Study: A Dose Escalation Study, with Serial Skin and Tumor Biopsies.
EVEREST STUDY: Erbitux + Irinotecan Dose Escalation Study. Group AClassic* Group B Dose Escalation q. 2nd Week until Skin Toxicity ≥ Grade 2 Group C Classic Skin toxicity≥ Grade 2 (~80) Irinotecan (Same Regimen) + Erbitux * Classic: Irinotecan + Erbitux 250 mg/m2 Irinotecan-Refractory mCRC 3 weeks Skin toxicity< Grade 2 (~80) Randomization n ~ 160 Tumor Biopsies Pre-Treatment Week 3 Only when Skin Toxicity Occurs (Group C) Primary endpoint: Difference in Expression of EGFR and other Downstream Signaling Pathway Markers in Skin Biopsies
Akt Can We Find Other Parameters to Predict Response to Cetuximab? SKIN TUMOR Biomarker Assays 1 2 Grb2 pEGFR pEGFR Sos K K Shc Shc Grb2 Sos PI3K Ras PTEN Raf pMAPK pMAPK GSK-3 MEK1/2 FKHR mTOR Bad MAPK p27 pAkt D1 Cyclin Cell cycle progression Proliferation Survival p27 p27
Cetuximab in Head and Neck Cancer. 1. Experience with Cetuximab in the first-line treatment of recurrent and/or metastatic SCCHN 2. Experience with Cetuximab in the treatment of recurrent and/or metastatic SCCHN refractory to platinum-based CT 3. Results of an international phase III study of radiation ± Cetuximab in patients with locoregionally advanced Head and Neck Cancer.
Cetuximab/Cisplatin or Cisplatin/Placebo in First-Line Treatment Advanced Head and Neck Cancer: Safety (Grades 3/4) Burtness et al. Clin Cancer Res 2003;9: 6088S.
Cetuximab in Combination with Cisplatin / 5-FU or Carboplatin/5-FU: Safety (Grades 3/4). Humblet et al. Proc Am Soc Clin Oncol 2004; Abstract 5513.
Results of an International Phase III Study of Radiation ± Cetuximab in Patients with Locoregionally Advanced Head and Neck Cancer. Paul Harari, Jordi Giralt, Nozar Azarnia, Patricia Molloy, Roger Cohen, David Raben, Christopher Jones, Merrill Kies, Jose Baselga, Kian Ang, James Bonner. Harari P et al. Proc Int Conf Head Neck Cancer 2004, abstract s087.
Cetuximab + RT RT Overall survival Efficacy: Survival Harari P et al. Proc Int Conf Head Neck Cancer 2004, abstract s087.
Erbitux + RT RT Locoregional control Efficacy: locoregional control Harari P et al. Proc Int Conf Head Neck Cancer 2004, abstract s087.
Most common adverse events # Listed for its relationship to Erbitux * p < 0.05, ** p < 0.001, Fisher’s exact test Harari P et al. Proc Int Conf Head Neck Cancer 2004, abstract s087.
Side Effect Profiles of Targeted Therapies Source: Summary of Product Characteristics for Bevacizumab and Cetuximab