Download
1 / 76
760 likes | 768 Views
This course discusses the role of bone marrow transplantation in large radiation incidents, covering scenarios, secondary triage, treatment options, and what the EBMT can offer in such events.

E N D
4th International Expert Course on the Medical Management of Radiological and Nuclear Events Stockholm 15-17th May 2013 The Place Of Bone Marrow Transplantation in Large Radiation incidents Prof Ray Powles Chairman European Blood Marrow Transplant EBMT Nuclear Accident Committee Head Haemato-oncology Cancer Centre London
European Blood and Marrow Transplant EBMT Nuclear Accident Committee • `Formed after 9/11 because it was proposed to the EBMT Board.... ............that our 500 BMT Centres may be a useful resource in the event of a massive terrorist radiation incident
EBMT Network • All 500 BMT centres in 27 EU countries • World Health Organisation (Collaborating Centre • IAEA • United States Radiation Injury Treatment Network (RITN) Memorandum of Understanding (MUO) • Since Fukushima......extending network • India Pakistan • Saudi Iran Israel • China Taiwan Japan Korea • Russia USA
Plan of the Talk • Scenarios • Secondary Triage • Treatment • Allografting • Autografting • RDD • What can the EBMT offer
Possible Large Scenarios100-3000+ victims • Nuclear Power station Failure Fukushima Cherobyl • Terrorist incidents
Radiation Exposure Devise • RED – Radiological Exposure / Emplaced Device • Taking a physically small but intense radioactive source and putting somewhere to expose people
Attack on a Nuclear Site • Taking something ‘large and energetic’ and impacting it on a nuclear site • Nuclear reactors are incredibly strong • A nuclear explosion is technically impossible
Improvised Nuclear Device • Needs resources of a nation state to produce a feasible nuclear weapon (Iran) • But with enough correct material and knowledge an improvised device could be made with a much lower yield
The U.S. government is planning to respond to a 1 and 10 kiloton (IND) improvised nuclear device (terrorist nuclear bomb) Affected Population
So lets go into more detail how EBMT can help in a major radiation incident
the key to primary triage Covert (obvious)......1/ move from source 2/ then decontaminate 3/ assess acute co-morbidities Overt (hidden)............ more complex? 1/ Disseminated from Metro incident 2/ Atom Bomb Flee in chaos from fall-out zone
Structural, radiation and medicalresponse zones RTR – Radiation TRiage, TReatment, TRansportation, TRansplantation
Plan of the Talk • Scenarios • Secondary Triage • Treatment • Allografting • Autografting • RDD • What can the EBMT offer
Secondary triage • How do we identify a group of irradiated patients that will develop bone marrow failure • In whom treatment can savethem? i.e. NOT those who will die anyway, or have had minimal irradiation
Biological Dosimetry Assays Not logistically feasible for large radiation incidents But a few marker patients might map out picture of dose distribution • Cytogenetic Assays currently available and calibrated: • Dicentrics • Micronuclei • FISH translocations • Premature chromosomal condensation • Others ‘on the near horizon’: • Serum biomarkers • γH2AX foci • genomic markers David Lloyd - HPA
Tokaimura Accident • September 30th 1999 • 3 victims exposed to substantial amount mixed neutron/photon ionizing irradiation • 2 received stem cell transplantation (matched sister and cord blood) within 10 days • Both engrafted with mixed chimerism • Both died (83 and 211 days) of multi-organ failure
Wall B A C W Floor
Prodromal Symptoms of Three Workersat the Tokai-mura accident Worker A 8Gy+ Nausea, Vomiting Diarrhea Loss of consciousness High fever (38.5 ℃) < 10 min < 60 min last for 10-20 sec Worker B 6Gy+ Nausea, Vomiting ≒1 hr a few hr Worker C 2-3GY Nausea
Clinical PictureTokaï-Mura Accident ( Japan 1999) 8Gy+ Aplasia Hemophagocytosis PBSCT Haematopoietic syndrome GI bleeding Diarrhoea Gastrointestinal disease Erythema, Blister Massive exudate Cutaneous syndrome Lung disease Lung oedema Renal Failure Liver dysfunction 1 2 3 4 5 6 7 8 9 10 11 Time after irradiation (weeks) Death
General Principles for ‘Accidental’ exposure to irradiation Small numbers of victims ? Contamination Inhalation Other injuries HETEROGENEOUS EXPOSURE. Great difficulty working out dose Since 1945……at least 800 victims with Acute Radiation Sickness in …….. 70 instances
Biological effects of accidental irradiation • Prof Ted Fleidner WHO REMPAN Centre Ulm • SEARCH programme • Since 1945 found 800 radiation victims in 70 incidents worldwide • He devised a scoring system to determine clinically whether the victim would • a/ die regardless of any treatment • b/ survive if appropriate treatment given • c/ not need any treatment
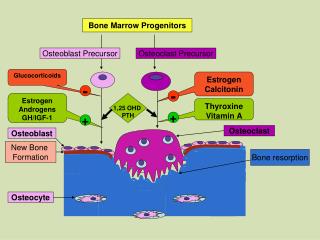
Initial (1st 48 hrs) Biological effects of irradiation • Haematological • Cutaneous • Gastrointestinal • Central nervous system
But a new approach was needed if a very large incident occurred
EBMT Consensus Pocket Guide • On EBMT Website.......... ...........Google EBMT and go to NAC
Organ specific checklists Blood count anytime L: Reference value: (1.5-4) x 109/l G: Reference value: (4-9) x 109/l T: Reference value: (140-400) x 109/l T.M. Fliedner et al., Br J Radiol. 2001
Granulocyte/Platelet changes in 17 patients characteristic for Grade H4 (essentially irreversible damage of stem cell pool) Courtesy: Prof T Fliedner
the key to secondary triage • ........firstly do leukocyte counts. • Secondarily........clinical manifextations
Summary of Pocket Guide • Score 1.... no treatment needed (less than 1Gy?).... • Score 2.....support only (2Gy-5Gy?) • Score 3... stem cell transplant....... (6Gy-9Gy?)......... • BUT it is the clinical score that counts, not the dose estimation
Plan of the Talk • Scenarios • Secondary Triage • Treatment • Allografting • Autografting • RDD • What can the EBMT offer
Treatment • In a pragmatic world the key to treatment is not bone marrow transplantation • Give marrow failure support......antibiotics etc
Haemopoetic support • Almost exactly the same as for treating AML, or Aplastic Anaemia.. • Clean single room with clean air • Washing hands etc • Antibiotics • Antifungals • Antivirals • Blood Products • And........immunoglogulins etc
Plan of the Talk • Scenarios • Secondary Triage • Treatment • Allografting • Autografting • RDD • What can the EBMT offer
Indications for transplant(allotransplantation) • Background.........previous attempts
Biological effects of accidental irradiation • Prof Ted Fleidner (SEARCH) • Since 1945 found 800 radiation victims in 70 incidents worldwide • Of these found 48 patients from 14 radiation incidents receiving haemopoetic stem cell transplants
Radiation Accidents from 1958-1999(48 transplants, 14 incidents): ~20 yrs old Location Date # ARS Victims # HSC HSC source Vinca, YU 10/15/58 6 5 marrow Obnisnsk, RU 11/2/62 1 1 marrow Arzamas,RU 3/11/63 2 1 marrow Pittsburgh, US 10/2/67 3 1 marrow Sungul, RU 4/5/68 2 2 marrow Chelyabinsk,RU 12/10/68 2 2 marrow Sormovo, RU 1/18/70 5 2 marrow Moscow, RU 5/26/71 4 3 marrow Shanghai, CN 9/1/80 1 fetal liver cells Chernobyl, UA 4/26/86 234 22 marrow, fetal Kaifun, CN 5/26/86 2 1 fetal Sor-Van, IS 6/21/90 1 1 marrow Shanghai, CN 6/25/90 4 4 marrow, liver Tokai-Mura, JP 9/30/99 3 2 peripheral blood, liver Courtesy: Prof Fliedner
48 Stem Cell Transplants 23/48 (48%) died post transplant within within 50 days 9 had evidence of ‘engraftment’ 16 patients had evidence of autologous recovery Death due to multi-organ failure. Transplant related or acute radiation?
Possible Mechanisms for MOF in Radiation Paralysis of Cell-Mediated Immune Responses (Excessive) Systemic Inflammatory Response Syndrome (SIRS) Systemic Inflammation Sepsis Multiple Organ Failure From Dr Makoto Akashi High-dose Radiation Bleeding Bone Marrow Failure Infection Tissue Damage Disturbance in Microcirculation Endothelial Cell Damage MODS Parenchymal Cell Damage ( Loss of electrolytes )
HSCT for Acute Radiation Syndrome Non-myeloablativeregimen, EBMT NAC HSCT Fludarabine 30mg/m2 ATG 2 mg/m2 -3 -8 -7 -6 -5 -4 -2 -1 0 +14 +21 +100 +180 CSA ( level>150µg/L) - 3 to > +100 MMF (30mg/kg/day)- 3 to + 30 • Eligibility: • Sibling • Unrelated • Cord G-CSF In some protocols
Ann Intern Med 2009; 150:132-138 Choosing an allocation model is a huge challenge
Stem Cell Transplantation ? Never an emergency! Not if MODS Always consider heterogeneity of irradiation and possibility of autologous hematopoietic recovery. Immediate typing Transplant - never before day 14-21 Low immunosuppression: fludarabine ± ATG CSA+MMF. No MTX High cell dose
Pocket Guide Indications for transplant(allotransplantation) • Wait 14-21 days of G-CSF treatment • No co-morbidity • potential donor • Score 3 pocket guide (no circulating neutrophils)
Plan of the Talk • Scenarios • Secondary Triage • Treatment • Allografting • Autografting • RDD • What can the EBMT offer
Indications for autologous transplant • Questions....... • Is multi-organ failure an inevitable consequence of accidental irradiation? • Does autografting makes a difference? i.e. Workers that have stem cells taken before exposure
Background to Fukushima • March 2010 • EBMT mobilized 120 centres in 48 hrs (a further 72 centres agreed to store autologous SC) Current situation at Fukushima..... • Sources still uncontrolled
Members UK Steering Committee • Penny Bevan • Ray Powles • Anthony Bleetman • Bhawna Sirohi • Celia Kendrick • Darren Walter • David Marks • David Temperton • Hilary.Walker • Lesley Prosser • Margaret Spittle • Monika Temple • Richard Rackham nhsbt. • Tony Pagliuca • Verity Kemp • David Brown • Corinne Perry • Chris Hayes
The Place of collecting autologous stem cells after a large radiation incident • Huge controversy after Fukushima Should we collect and store Stem Cells from workers? who may subsequently need to go near a radioactive source to neutralize it? • EBMT NAC meeting March 2011 • EBMT NAC meeting June 2011 • COSTEM July 2011