Download
1 / 79
891 likes | 1.29k Views
Chapter 4 Nutrition During Pregnancy. Nutrition Through the Life Cycle Judith E. Brown. Introduction. Topics covered include: Status of pregnancy outcome Reducing infant mortality and morbidity Physiology of pregnancy Embryonic & fetal growth and developmen Pregnancy weight gain

E N D
Chapter 4Nutrition During Pregnancy Nutrition Through the Life Cycle Judith E. Brown
Introduction • Topics covered include: • Status of pregnancy outcome • Reducing infant mortality and morbidity • Physiology of pregnancy • Embryonic & fetal growth and developmen • Pregnancy weight gain • Nutrition and course/outcome of pregnancy • Nutrient needs during pregnancy
Introduction • Topics covered include: • Exercise and Pregnancy • Food Safety issues during pregnancy • Common Health Problems during pregnancy
The Status of Pregnancy Outcomes • Infant mortality: • Reflects general health status of a population • Decreases in mortality related to improvements in social circumstances, safe & nutritious food supply, & infectious disease control
Natality Statistics: Rates, Definitions, and Trends in the Rates in the United States
Differences by Race http://www.cdc.gov/nchs/data/databriefs/db09.htm
Chronology of Events Related to Declines in Infant Mortality in the United States
Low Birthweight, Preterm Delivery, and Infant Mortality • Low birth weight or preterm infants at high risk of dying in 1st year of life • 8.2% of births are LBW yet comprise 66% of infant deaths • 12.7% are born preterm yet account for high incidence of infant deaths
Reducing Infant Mortality and Morbidity • Improve birth weight of newborns • Desirable birth weight = 3500-4500 g (7 lb. 12 oz.-10 lb.) • Infants born with desirable wt are less likely to develop: • Heart and Lung diseases • Diabetes • Hypertension
Health Objectives for 2010 for the Nation Related to Pregnant Women and Infants • The Health Objectives for 2010 in relation to pregnant women and infants focus on • The reduction of low birth weight, • Preterm delivery • Infant mortality • A number of the objectives are related to nutrition
Health Objectives for 2010 for the Nation Related to Pregnant Women and Infants • Nutrition related objectives: • Reduce anemia in pregnant females • Reduce incidence of spina bifida • Increase abstinence form alcohol use and reduce the incidence of fetal alcohol syndrome • Increase appropriate weight gain during pregnancy
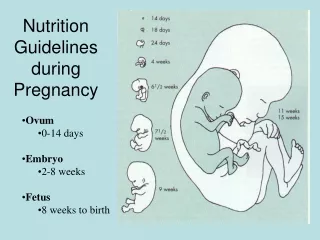
Physiology of Pregnancy • Key terms: • Gestational age • Assessed from date of conception • Average pregnancy is 38 weeks • Menstrual age • Assessed from onset of last menstrual period • Average pregnancy is 40 weeks
Maternal Physiology • Changes in maternal body composition & functions occur in specific sequence
Normal Physiological Changes during Pregnancy • Two phases of changes: • Maternal anabolic changes • Takes place in the 1st half of pregnancy • Maternal catabolic changes • Takes place in the 2nd half of pregnancy
Body Water Changes • Body water • Increases from ~7 L to 10 L • Results from increased blood and body tissues & extracellular volume & amniotic fluid • Edema • Swelling due to accumulation of extracelluar fluid
Maternal Nutrient Metabolism • Changes can be seen in the first few weeks after conception. • Ensures that nutrients will be available to the fetus when needed.
Carbohydrate Metabolism • Glucose is preferred fuel for fetus • “Diabetogenic effect of pregnancy” results from maternal insulin resistance
Carbohydrate Metabolism • Early pregnancy: • High estrogen & progesterone stimulate insulin which increases glucose glycogen & fat • Late pregnancy: • Human chorionic somatotropin (hCS) & prolactin inhibit conversion of glucose to glycogen & fat
About 925 g of protein accumulate during pregnancy Protein & amino acids conserved during pregnancy No evidence the body stores protein early in pregnancy Needs must be met by mother’s intake of protein Protein Metabolism
Fat Metabolism • Fat stores • Accumulate in first half of pregnancy • Enhanced fat mobilization in last half • Blood lipid levels increase • Increased cholesterol is substrate for steroid hormone synthesis
Mineral Metabolism • Calcium • Increased bone turnover & reformation • Sodium • Accumulation in mother, placenta, & fetus • Restriction of sodium potentially harmful
The Placenta • Functions: • Hormone & enzyme production • Nutrient & gas exchange • Remove waste from fetus • Structure: • Double lining of cells separating maternal & fetal blood
The Placenta • Nutrient Transfer • Factors that affect the transfer: • Size and charge of molecules • Small molecules pass through most easily • Lipid solubility of particles • Concentration of nutrients in maternal and fetal blood
The Placenta • Nutrient Transfer • The fetus is not a parasite • Nutrients first used for maternal needs, then for placenta & last for fetal needed • The fetus is harmed more than the mother by poor maternal nutrition
Embryonic and Fetal Growth and Development • Growth and Development • Is at the highest level during the 9 months of gestation • If rate gain continued at this level, at 1 year of age the infant would be 160 lbs. • Table 4.12 provides an overview of embryonic and fetal development during pregnancy
Critical Periods of Growth and Development • Differentiation • Cellular acquisition of one or more characteristics or functions different from that of the original cell • Critical Periods • Preprogrammed time periods during embryonic & fetal development when specific cells, organs & tissues are formed & integrated or functional levels established
Critical Periods of Growth and Development • Four periods of growth & development 1) Hyperplasia( cell multiplication) 2) Hyperplasia & hypertrophy 3) Hypertrophy( cell growth) 4) Maturation (stabilization of cell number & size)
Variation in Fetal Growth • Variations linked to: • Energy, nutrient, & oxygen availability • Genetically programmed growth & development • Insulin-like growth factor (IGF-1) is main fetal growth stimulator
Newborn Weight Classifications • Terms to describe newborn size • SGA (small for gestational age) • dSGA (disproportionately small for gestational age) • pSGA (proportionately small for gestational age) • LGA (large for gestational age) • Ponderal Index (similar to BMI) • Calulated by wt in g divided by cube of lt times 100 • PI for normal wt ~23-25
Nutrition, Miscarriages and Preterm Delivery • Miscarriages • Thought to be caused by genetic, uterine, or hormonal abnormalities • Preterm Delivery • Infants born preterm are at risk for death, neurological problems, congenital malformations, & chronic health problems
Fetal-Origins Hypothesis of Later Disease Risk • Theory that exposures to adverse nutritional & other conditions during critical or sensitive periods of growth & development can permanently affect body structures & functions • Changes may predispose individuals to CVD, type 2 diabetes, hypertension, & other disorders in later life
The Fetal-Origins Hypothesis • Mechanisms underlying the fetal origins hypothesis • Influenced by genes • Also influenced by environmental exposure (in utero) • AKA developmental plasticity • Concept that the development can be modified by particular environmental conditions experienced by a fetus or infant
The Fetal-Origins Hypothesis • Environmental Exposures • Modify development • Epigenetic mechanisms • Epigenetics (epi=over, above) • Biological mechanisms that change gene function without changing the structure of DNA. Epigenetic mechanisms are affected by environmental factors.
The Fetal-Origins Hypothesis • Nutrition programming • Fetal exposure to certain levels of energy & nutrients modify function of genes in ways that affect metabolism & development of diseases in later life • Limitations of the fetal-origins hypothesis • Unanswered questions • What levels are related to changes? • What exposures?
Pregnancy Weight Gain • Weight gain during pregnancy is related to the weight and health status of the newborn infant • Recommendations for weight gain during pregnancy is found in Table 4.17 • Recommendations for weight gain are influenced by the pre-pregnancy status of the mother
~2-5 pounds in first trimester Gradual & consistent gains thereafter Rate of Pregnancy Weight Gain
Composition of Weight Gain • The fetus is only about 1/3 of the total weight gain • The balance of the weight gain is related to body fat changes, placenta, amniotic fluid, increase of extracellular fluids, and blood supply of the mother
Postpartum Weight Retention • Much concern over pregnancy weight gain and long-term obesity • ~15 pounds lost at delivery • Wt loss difficult in women who gained >45 pounds or with low activity levels • Women with recommended wt gain in pregnancy are ~2 pounds heavier at 1 yr postpartum • Lactating women lose slightly more
Nutrition and the Course and Outcome of Pregnancy • Famine and pregnancy outcome • The Dutch Hungerwinter, 1943-1944 • Decline in pregnancy rates • Lower birth weights • The siege of Leningrad, 1942 • Increase in infertility & low birth weights • Infant death rates increased • Food shortages in Japan • Similar to the outcomes found in Holland and Leningrad above
Nutrition and the Course and Outcome of Pregnancy • Contemporary prenatal nutrition research results • “Good nutritional status maintained before and throughout pregnancy decreases the risk of birth defects, suboptimal fetal growth and development, and chronic health problems later in life.”
Nutrient Needs During Pregnancy • Nutrient needs vary during the course of the pregnancy • Overall, nutrient needs can be met with well balanced, adequate and healthful diets consisting of basic foods
Nutrient Needs During Pregnancy • Energy requirements in pregnancy • ~300 additional cal/d • +340/d in 2nd trimester +452/d in 3rd trimester • Assessment of caloric intake • Most easily assessed by pregnancy weight gain • As long as there is no noticeable edema
Carbohydrates, Artificial Sweeteners and Alcohol • Carbohydrate intake (50-65%) • Basic foods such as • vegetables, fruits, and whole grains with fibers = best choice • Artificial sweeteners • No scientific evidence of harm • Alcohol ingestion • Strongly advised to avoid during pregnancy