Download
1 / 34
350 likes | 473 Views
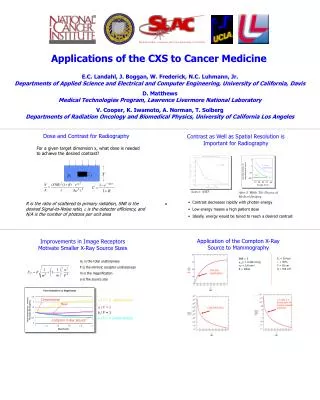
Customized Cancer Medicine. All Treatments are Customized at the point of delivery All Treatments Are Designed to Take advantage of Differences between Cancer Cells and Normal Cells

E N D
Customized Cancer Medicine All Treatments are Customized at the point of delivery All Treatments Are Designed to Take advantage of Differences between Cancer Cells and Normal Cells Some of these differences are Generic and some are more Specific to the Type of Cancer, the Subtype, or even to the Individual Person
Customized Cancer Medicine Generic Treatments Cancer Starts from One Cell in One Place Surgery- Early Detection Cancer Cells Divide Faster Chemotherapy and Radiotherapy Cancer Type Specific Treatments Hormone Responsive Prostate/Breast Tissue Type Thyroid Receptors Monoclonal Antibodies
Customized Cancer Medicine Personalized Treatments Not All People Are The Same Match The Treatment For the Person’s Inherited Genes Pharmacogenomics Not All Tumors Are The Same Match The Treatment For the Tumor That Person Has Tumor Phenotyping Gene Expression Profiling The Relationship between the Immune System of the Person and Their Tumor Is Variable Re Educate the Immune System Monoclonal Antibodies Transplanted Immune Cells Tumor Vaccines
B cell T cell Two Arms of the Immune System B cells T cells foreign substance (antigen) antibody Abnormal cell Function: Make Antibodies Kill abnormal cells
transformation Normal B cells B lymphoma cells Lymphoma Tumors Have A Special Target
Monoclonal Antibody Therapy Custom Made Anti-idiotype antibody Tumor Idiotype Lymphoma B cell
New England Journal of Medicine, 306:517. 1982 Treatment of B Cell Lymphoma with Monoclonal Anti Idiotype Antibody Richard A Miller, David G. Maloney, Roger Warnke, and Ronald Levy
Monoclonal Antibody Therapy Once Size Fits All Anti-idiotype antibody Tumor Idiotype Rituximab Lymphoma B cell CD20
Aren’t antibodies wholesome, natural and without side effects
Rituximab Anti-tumor Effect: Proposed Mechanisms 1) Apoptosis, Anti-proliferation 2) Complement-mediated Killing Tumor Cell T Cells CD20 or other tumor Ags FcR Natural Killler Cells Monocytes FcR Dendritic Cells 3) Antibody-dependent Cellular Cytotoxicity (ADCC) 4) Antigen Presentation and Cross-priming
Rituximab Clinical Response Determined by Genetics FcgR IIIA 158 V/F polymorphism V/V V/F F/F F Carriers 8/10 12/28 9/23 21/51 (80%) (43%) (39%) (41%) p=0.037
Monoclonal Antibody Conclusions Antibodies are Effective Drugs Improved versions will be Found New Targets will be Found New Disease Indications Will be Found ? Mechanisms of Action and Resistance ? Prediction of Efficacy
A Therapeutic Vaccine for Lymphoma “Rescue hybridization” Myeloma cell + Tumor Biopsy . Vaccine Production 3 2 1 Immunization Tumor Id Protein KLH carrier protein Id Adjuvant (SAF)
Genitope Phase III Trial Treatment Schedule Enrollment Monthly Vaccines x7 Randomize 2/1 Recovery 26 weeks Immunization: 28 weeks CVP Follow for Time to Progression
Idiotype Vaccine Can A Custom Vaccine Be Practical?
Idiotype Vaccine Production Via Recombinant DNA Recombinant Id proteins Genetic Id Vaccines Naked DNA Recombinant Viruses Mammalian or insect cells Bacteria Plants Cell Free Immunoglobulin Fragments Whole Immunoglobulin
3 2 1 1. Lymphoma Biopsy Vaccine Just in Time 2. Amplify Ig V genes Insert into Vector (~ 3 Days) 4. Vaccinate 3. Express Cell-Free /Purify (~ 2 days)
Customized Cancer Medicine Personalized Treatments Are Problematic Drug Industry Mass produced products for mass markets High margins between cost of goods and sales price Intellectual Property favors composition over use Health Care Delivery Organizations Standard Operating Procedures Risk/Reward better for acute interventions HMO model shifts financial risk to the provider Regulatory Bodies Accustomed to manufacturing issues and large scale trials Privacy Concerns Work against genetic testing Work against use of medical records to develop predictive tests
Future Doctor “Take some immunotherapy and call me in the morning”
Using The Immune System To Treat Cancer: 2005 Antibodies, Antibodies and more Antibodies Therapeutic Vaccination Dendritic Cells Adoptive Cellular Therapy Allogeneic Bone Marrow Transplantation Autologous T Cells Inhibition of Suppressor T Cells
Dendritic Cells • Most potent “antigen-presenting cells” • Reside in tissues to collect antigen -> travel to lymph nodes • Co-culture with antigens -> cellular vaccine
1 2 Myeloma cell + Fusion TumorBiopsy Vaccine Production Leukapheresis + Immunization 4 Dendritic Cells Tumor Id Protein Antigen-Pulsed Dendritic Cells Co-culture 3
Idiotype-pulsed dendritic cell vaccination Pre-vaccine 11 months post-vaccine
In situ Vaccination with DC Chemotherapy 2 Leukapheresis 3 1 Intratumor Injection Dendritic Cells
100 80 60 PROBABILITY (%) Responders (n=14) p<0.0001 40 non-Responders (n=18) 20 0 0 2 4 6 8 10 TIME (YEARS) Freedom From Progression Follicular Lymphoma first remission
240 220 200 180 160 140 120 100 80 60 40 20 0 Rituximab Publications 200 180 Publications 160 Genentech (DNA) stock price 140 Number of publications IDEC (IDPH) stock price 120 Stock price ($) 100 80 60 40 20 0 00 93 94 Jan/91 92 97 98 99 95 96 Year Pivotal trial results FDA approval 1st clinical trial
3 days 4 hours 6 days Abdominal SPECT Abdominal CT Monoclonal Antibody Imaging 111In-Labeled Zevalin™ 106-00-158RS
Antigen Cells Fuse into a Hybridoma Cancerous Plasma Cell Antibody-producing Plasma Cell Monoclonial Antibodies Hybridoma TechnologyMaking Antibodies Immortal