Download
1 / 44
440 likes | 561 Views
Table 1. Comparison of laboratory investigations using the conventional approach and the LAS (Clin Chem 45:8 1168-1175 (1999) Conventional LAS Results Mean number of tests ordered 32.7 17.8 t -Test for two related samples t = 5.4, P <0.01

E N D
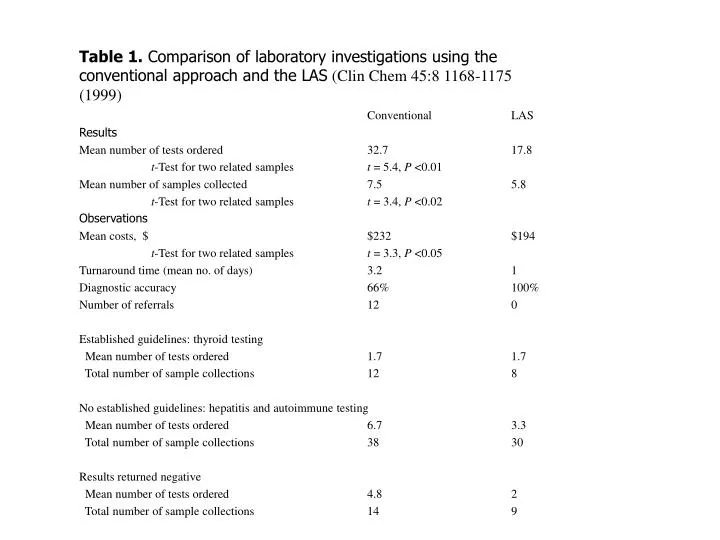
Table 1. Comparison of laboratory investigations using the conventional approach and the LAS (Clin Chem 45:8 1168-1175 (1999) Conventional LAS Results Mean number of tests ordered 32.7 17.8 t-Test for two related samples t = 5.4, P <0.01 Mean number of samples collected 7.5 5.8 t-Test for two related samples t = 3.4, P <0.02 Observations Mean costs, $ $232 $194 t-Test for two related samples t = 3.3, P <0.05 Turnaround time (mean no. of days) 3.2 1 Diagnostic accuracy 66% 100% Number of referrals 12 0 Established guidelines: thyroid testing Mean number of tests ordered 1.7 1.7 Total number of sample collections 12 8 No established guidelines: hepatitis and autoimmune testing Mean number of tests ordered 6.7 3.3 Total number of sample collections 38 30 Results returned negative Mean number of tests ordered 4.8 2 Total number of sample collections 14 9
Generate Rule Search Rule List RULE EXISTS Search comment List NEW RULE Enter new Comment Retrieve Comment Update rule list Modify if required Update comment list Search Rule List Enter Data
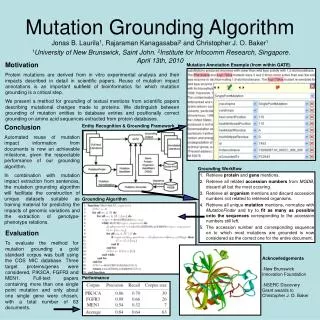
Qualitative Gender Clinical details Drug therapy Quantitative Age Total T4 TSH Free T4 Free T3 Variables UsedTFT application
Decision Range >=60 >=20; <60 >=10; <20 >5; <10 >4; <=5 >=0.4; <4 >=0.25; <0.4 <0.25 Description Markedly high Very High High Mildly raised Near URL Normal Near LRL Below detection limit Adult decision rangesTSH (mu/L)
CLINICAL DETAILS A. Suspected hyperthyroidism B. Suspected hypothyroidism C.Post Radioiodine therapy D. Post thyroid surgery E. On thyroxine treatment F. On T3 treatment G. On Carbimazole H. On PTU Z. Non-specific DRUG THERAPY A. Lithium B. Oestrogens C. Amiodarone D. Beta-blockers E. Glucocorticoids F. Phenytoin G. Carbamazepine H. Androgens Z. No relevant drugs Clinical and Drug detailsTFT
Variables UsedProtein electrophoresis • Quantitative • patients age • serum total protein, albumin, -globulin, paraprotein concentrations • Semi-quantitative • Visual assessment of albumin, 1,,2,, 1,,,,2,, and concentrations • Qualitative • patients gender • Visual inspection of zones and interzones (11 variables), e.g. 1 zone,- interzone findings
Performance evaluation - TFTPercentage of automatically assigned interpretations (AAI) per TFT batch
TFT application statistics • Number of variables specified: 8 • Number of options/decision levels: 70 • Number of theoretical data combinations: 20,412,000 • Number of cases entered via primer knowledge bases: 1142 • Number of rules: >2900 • Percentage of automatically assigned interpretations [using the primer knowledge bases] • At the outset: 66% • After the first 500 patient cases: 70% • Maximum achieved: 95% • Number of interpretations rejected: <1%
electrophoresis application statistics • Number of variables specified: 23 (22 used in rule generation) • Number of options/decision levels: 183 • Number of theoretical data combinations: 8,800,000,000,000,000,000 • Number of cases entered via primer knowledge bases: 206 • Number of rules: 350 • Percentage of automatically assigned interpretations [using the primer knowledge bases] • At the outset: 78% • After the first 500 patient cases: 72% • Maximum achieved: 70-80% • Number of interpretations rejected: 0
Clinical evaluationTFT application(27 TFT requests on 15 randomly-selected new referrals to a thyroid clinic were studied; 2 evaluators participated)
Clinical evaluationElectrophoresis application(115 questionnaires circulated, 64 returned, 56% response)
Clinical evaluationElectrophoresis application(115 questionnaires circulated, 64 returned, 56% response)
Performance evaluationElectrophoresis application(to demonstrate knowledge acquisition)
Cooperativity DATA KBS Interpretation Diagnostic outcome
Diagnostic outcome (2) Diagnostic outcome (4) Diagnostic outcome (3) KBS-2 KBS-4 KBS-3 Comment Comment Comment Cooperativity KBS-i Diagnostic outcome (1) KBS-1 Comment Integrating Comment
CooperativityOrgan-related profiles • Renal profile • Na, K, Urea, Creatinine • Bone profile • Ca, Alb, Corr Ca, Phosphate, AlkPhos • Liver profile • Bili, Alb, T Protein, AST, Alk Phos, GGT • Cardiac profile • Lipid profile
140 mmol/L 130 mmol/L CooperativityDecision Levels 160 mmol/L 150 mmol/L Plasma Sodium Concentration 120 mmol/L 110 mmol/L
Rule Elements Rules and rule elements Diagnostic outcomes Comments R Tr L Tl B Tb C Tc Integrating rule and its elements i Age Sex Clin Ti
PRIMER Renal KBS PRIMER Bone KBS PRIMER Liver KBS PRIMER Cardiac/ Lipid KBS CooperativityPrimer knowledge bases Universe KBS (Primers are subsets)
Renal profile prerenal impairment Renal impairment hyponatraemia hypokalaemia hypernatraemia hyperkalaemia etc Bone profile osteomalacia pattern renal osteomalacia primary hyperparathyroidism etc Selected Diagnostic Outcomes
Renal Na 133 [Low] K 5.8 [Raised] Urea 30.5 [raised] Creatinine 400 [Raised] Interpretation Renal impairment with hyperkalaemia and mild hyponatraemia Diagnostic outcome renal impairment Bone Ca 1.94 Corr Ca 2.04 [Low] Alb 35 [Normal] Phosphate 1.88 [High] Alk Phos 450 [High] Interpretation Hypocalcaemia, raised phosphate and Alk Phos: osteomalacia pattern Diagnostic outcome osteomalacia pattern Profile interpretations
Cooperative KBS output • Renal KBS comment • Renal impairment with hyperkalaemia and mild hyponatraemia. [DO= renal impairment] • Bone KBS comment • hypocalcaemia, raised phosphate and Alk Phos. DO = osteomalacia pattern. • Integrating KBS comment • These results are consistent with renal failure and associated renal osteodystrophy
Decision Support SystemsSupport for Health Care Professionals
Decision Support SystemsSupport for Health Care Professionals • Microbiology Applications • Computerised infectious disease monitor (Evans, 1986). Computer-generated alarms were produced for (1) all patients with hospital-acquired infections; (2) patients on antibiotics to which they were not susceptible; (3) who could be receiving less expensive antibiotics; (4) who were receiving prophylactic antibiotcis for too long. Use of the system saved time for hospital infection control staff, and improved antibiotic use. • MRSA monitor (Safran, Scherrer 1994). Infection control nurses were provided daily with computer-generated lab alerts giving details of MRSA+ together with re-admission alerts giving details of new admissions previously known to be colonised with MRSA. System saved time for ICNs and helped as a preventive warning.
Decision Support SystemsSupport for Health Care Professionals • Histopathology/Cytopathology applications • PAPNET Cervical Screening Neural Network • Telepathology
Decision Support SystemsSupport for Health Care Professionals • Haematology applications • Diamond and Nguyen/Coulter Electronics. Various DSS applications for use with Coulter systems, flow cytometry, classification of haematological malignancies etc.
EQA Applications • EQA Toolkit