Download
1 / 36
390 likes | 426 Views
Learn about the incidence, sites of metastases, survival rates, clinical vignettes, treatment philosophies, systemic therapies, and toxicities in metastatic breast cancer. Explore endocrine therapy, HER2 targeted therapies, and chemotherapy options.

E N D
METASTATIC DISEASEIN BREAST CANCER Mario Alberto Vásquez-Chaves, MD MsC Tokyo Women´s Medical University June 2011
WHAT IS METASTATIC BRCA? • Anything more distant than ipsilateral Axillar or Internal mammary LNs • may PRESENT with distant mets • may RECURR outside of this area
INCIDENCE • Between 5-10% metastatic at diagnosis • Majority = women relapsing with metastatic disease • Roughly 40,000 women die each year from metastatic BrCa
SITES OF METASTASES • Bones • Liver • Lungs • Brain • Peritoneal • LAD • Skin
SURVIVAL WITH MBRCA • Can be few months to years (Vogel et al, Cancer, 1992) • 15 - 90+ months • Depends on sites involved and rate of tumor progression • Volume of disease • Nonvisceral vs visceral • Receptor status (?HER2) • Response to Rx Yamamoto et al, JCO, 1998
MEDIAN OVERALL SURVIVAL ~ 2 years (26 months, Vogel JCO, 1992) NCDB, Five Year Survival Table for Cases Diagnosed in 1998 and 1999
CLINICAL VIGNETTE • 64 yo F presents with new dry cough, progressive over last several weeks • Stage IIB infiltrating ductal, HR+,HER2- diagnosed in 2002 • S/p lumpectomy, AC x4, XRT and 5 yrs of AI • 40 pack-yr history • Work up reveals….
SUSPECTED RECURRENCE…. • Establish diagnosis • ? Need to biopsy • 13-40% discordance in receptor status between primary tumor and metastasis • Restage • CBC, LFTs, imaging
DIAGNOSIS ESTABLISHED…. • Estimate prognosis • Burden and location of mets • Estimate likelihood of response to Rx • Disease free interval • Tumor factors • Establish goals of therapy
CURRENT TREATMENT PHILOSOPHY • MACROmetastasis = expression of systemic disease • Locoregional therapy • Appropriate if impending local complication • Palliative benefit • Generally, no improvement in survival Systemic medical therapy backbone of Rx
GOALS OF SYSTEMIC THERAPY Controlling disease • Palliation • Prolong survival ==> no prospective randomized clinical trials showing therapy extends survival over BSC “Cure” Greenberg et al, JCO, 1996 • 1581 pts with met BrCa • CR with therapy = 16% • Alive and still in CR at 5 yrs = 1.6%
“TREATABLE BUT NOT CURABLE” • Prolong survival with as few symptoms and side effects as possible…. • Data where available, often no head-to-head trials of the multiple therapies…. • OS remains gold standard
SYSTEMIC THERAPIES • Bisphosphonates • Endocrine therapies • HER2 targeted therapies • Conventional chemotherapy (cytotoxics) • Other biologics Toxicity
BISPHOSPHONATES • Reduction of bony complications (Thierhault et al, JCO, 1999) • Which agent? Zolendronate, pamidronate • When to start? 1st met, 1st bony met…. • Timing? q4wks, q3mos…. • When to stop??
PREDICTIVE FACTORS, RESPONSE TO HORMONAL THERAPY (TAMOXIFEN, ARIMIDEX) • McGuire et al, BCRT, 1987
AGENTS • Ovarian ablation/suppression • Hormone withdrawal • SERMs • Tamoxifen • Toremifene • Aromatase inhibitors • Steroidal: exemestane • Non-steroidals: anastrozole, letrozole • Estrogen receptor down-regulators • Androgens/estrogens/progestins • Megesterol acetate
ENDOCRINE THERAPY • Which patients? Low risk pt (HR-?) • How likely to respond? • 10-40% RR, SD 20-30% • For how long? • Response duration variable • When to use? Used early: low toxicity, good chance of response Wilcken N, Hornbuckle J, Ghersi D. Cochrane Database of Systematic Reviews 2003
ENDOCRINE THERAPY • What to use? • PRE: Tam vs ovarian suppression vs ??? • POST: AI > Tam for RR, OS, TTP (11% benefit in relative HR, Mauri, JCNI, 2006) • 2nd line: evidence for tam, fulvestrant, another AI • 3rd, 4th….. ??? • Combinations? • ET combos: tam+ovarian ablation, no study for AI + Tam in metastatic disease • ET + cytotoxics: likely no survival benefit(Fossati et al, JCO, 1998 )
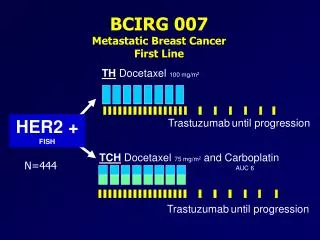
HR+ AND HER2+ • Conflicting evidence….. • TanDem Study • Median OS 28.5 months A+H 25.1 months A-->H 17.2 months A alone Clemens et al, ASCO Breast 2007, #231
PREDICTIVE FACTORS Vogel et al, JCO, 2002
HER2 TARGETED AGENTS • Trastuzumab (humanized, monoclonal Ab) • Lapatinib (small molecule, tyrosine kinase inhibitor [TKI] of EGFR and HER2) • Pertuzumab (monoclonal Ab, blocks dimerization of HER2/3) • CI-1033, pan-HER TKI
TRASTUZUMAB • Can use with or without chemo • Monotherapy: RR close to 30%, clinical benefit rate close to 50% (Vogel et al, JCO, 2002) • Combination: up to 63% RR, TTP 9 mos for docetaxel + tras, minimal add’l toxicity (Esteva et al, JCO, 2002) • When to stop? Slamon et al, NEJM, 2001
LAPATINIB • Capecitabine/lapatinib vs monotherapy • RR 22% vs 14%, p = 0.09 • TTP 8.4 vs 4.3 mos, p <0.0001 • OS not sig • Pts progressing on trastuzumab combined with capecitabine • Other combinations? • Monotherapy 1st line: RR 24%, TTF 16.1 wks (Gomez et al, JCO, 2007) Geyer et al, NEJM, 2006
ESTABLISHED AGENTS • Anthracyclines (doxorubicin, mitoxantrone, liposomal doxorubicin) • Anti-mitotics (taxanes, vinorelbine, ixabepilone) • Anti-metabolites (5FU, capecitabine, methotrexate) • Alkylators (cis/carboplatin) • Gemcitabine • Etoposide
CHEMOTHERAPY • Which patients? • When? Consider if (NCCN consensus-based): • Visceral disease with symptoms • Patients failing ET • Hormone receptor negative • Rapidly progressing?
SINGLE AGENTS • What to use first? No studies to suggest optimal sequence • What dose? No advantage to higher dose • Schedule? Weekly vs q3Wks, esp for taxanes (CALGB 9840) • How likely to respond? First line, RR 30-50% • Continuous vs intermittent? PFS prolonged, but probably not OS (Muss et al, NEJM 1991)
E2100 • Paclitaxel/bev vs paclitaxel wkly (first-line) • PFS 11.8 vs 5.9 mos • OS 26.7 vs 25.2 mos (NS) • RR 36% vs 21% • Grade 3+ CVAs 1.9% Miller et al, NEJM 2007
BEVACIZUMAB • AVADO study (ASCO 2008) • Doce/bev 15 or 7.5 vs docetaxel q3wk alone • RR 63.1% vs 55.2% vs 44.4% • PFS: 8.8 vs 8.7 vs 8.0 mos • HER2+ patients? (phase II, Pegram SABCS 2006) • Dose? • When to stop? • 2nd line? (Miller et al, JCO, 2005) • Combinations? (Xcalibur trial, RIBBON-1 and 2)
SUMMARY • Choose therapy MOST likely to work with LEAST toxicity • Monitor pt for response and toxicity • When to stop actively treating the cancer in mBrCa??? • Return to our patient: • Visceral mets • Symptomatic • ER+PR+ HER2- What’s the right therapy choice?