Download
1 / 46
500 likes | 1.01k Views
Infective Endocarditis. Airley E. Fish, MD Echo Conference January 16, 2008. Outline. Definition Epidemiology/Predisposing factors Microbiology Clinical manifestations Cardiac complications Diagnosis Indications for TTE vs TEE Treatment Indications for surgery

E N D
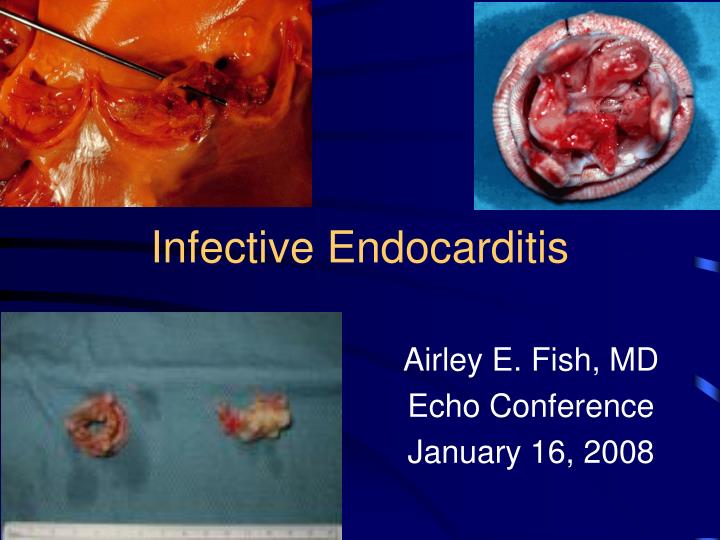
Infective Endocarditis Airley E. Fish, MD Echo Conference January 16, 2008
Outline • Definition • Epidemiology/Predisposing factors • Microbiology • Clinical manifestations • Cardiac complications • Diagnosis • Indications for TTE vs TEE • Treatment • Indications for surgery • Prognosis – mortality & relapse rates • Indications for antibiotic prophylaxis
Microbial infection of endocardium Vegetation Platelets Fibrin Microorganisms Inflammatory cells Definition Images from www.escuela.med.puc.cl
Vegetation – Gross & Microscopic Low power view of endocardium & myocardium, showing a fibrin vegetation on the endocardial surface. Endocardium appears edematous & inflamed Large, friable vegetation on the mitral valve Images from www.pathology.vcu.edu
Location Predominantly heart valves, but can occur on/in: Septal defects Chordae tendinae Mural endocardium Acute vs sub-acute/chronic Temporal Severity of clinical presentation Progression of untreated disease Definition
Factors altering immunity: Immunosuppression Diabetes Chronic alcoholism Structural cardiac abnormalities: AS, AR Bicuspid aortic valve MS, MR Senile mitral ring calcification Factors causing bacteremia: Dental work/Poor dental hygiene IVDU GU/GI procedures External factors: Mechanical valves Indwelling vascular catheters Pacing wires (IV) Conditions Predisposing to IE Modified from David M. Leder Echo Conference 01/07
Epidemiology/Predisposing Factors • IE of native valves • IE of prosthetic valves • Nosocomial IE
Epidemiology/Predisposing Factors – Native Valves • Incidence: 1.7-6.2 cases/100K person-years • Gender: ♂ predominance (1.7:1) • Age: > ½ of all cases occur in adults > 60 • ↓ in incidence of RHD in post antibiotic era • ↑ in elderly • ↑ degenerative valve disease • ↑ prosthetic valves • ↑ ‘ed exposure to nosocomial bacteremia • History of infective endocarditis • Recurrence in 4.5% of large cohort of non-addicts
Epidemiology/Predisposing Factors – Native Valves • Structural heart disease • ¾ of patients have preexisting structural cardiac abnormality • MVP most common • MVP + MR + thickened leaflets = 5-8 x risk IE! • Injection-drug use • Trend toward younger patients • Incidence of 150-2000 per 100,000 person years (higher if co-existent valvular disease) • Most significant risk factor for R-sided endocarditis • L-sided disease more common in addicts • S. aureus predominant organism • Vegetations often larger (i.e. > 1 cm) • Injection cocaine > other drugs
HIV infection S. aureus most frequent pathogen Unusual organisms (e.g. salmonella and listeria) ?Independent risk factor for IE in IVDA (unconfirmed) Other Pregnancy AV fistulas for HD Central venous and PA catheters Peritoneovenous shunts for intractable ascites Ventriculoatrial shunts for hydrocephalus Epidemiology/Predisposing Factors – Native Valves
Prosthetic heart valves 7-25% of cases (likely to ↑ with aging population) 1-4% of valve recipients during the 1st year after replacement 1% per year thereafter Risk IE mechanical > bioprosthetic 1st 3 months Equivalent risk @ 5 years Epidemiology/Predisposing Factors – Prosthetic Valves
Epidemiology/Predisposing Factors – Nosocomial IE • Nosocomial endocarditis • 7-29% of all 3° care hospital cases • Dx >72 hours after admission with no evidence of IE on admission or within 60 days of a prior admission if risk factor for bacteremia or IE during hospitalization • Complication of bacteremia 2° • Invasive intravascular procedure • IV catheter-related infection
S. aureus (32%) Viridans group streptococci (18%) Enterococci (11%) Frequently implicated in nosocomial bacteremia, but endocarditis rare Coagulase-negative staphylococci (11%) Most common pathogen in early prosthetic valve IE Culture negative endocarditis (8%) Streptococcus bovis (7%) Common in elderly Preexisting colonic lesions Other streptococci (5%) Other organisms (3%) Microbiology
Microbiology • Fungi (2%) • HACEK - fastidious gram negative bacteria (2%) • Haemophilus aphrophilus • Actinobacillus actinomycetemcomitans • Cardiobacterium hominis • Eikenella corrodens • Kingella kingae • Non-HACEK gram-negative bacteria (2%) • Polymicrobial (1%) • More common in association with IVDU
Clinical Symptoms • Fever (80%) • Anorexia (75%) • Chills (40%) • Dyspnea (40%) • Weight loss (25%) • Night sweats (25%) • Myalgias/arthralgias (15%) Adapted from Mandell et al 2000 (Karmpaliotis) and Leder Echo Conference 2007
Clinical Signs • Fever 90% • Heart murmur 85% • Changing murmur (5-10%) • New murmur (3-5%) • Peripheral manifestations 50% • Petechiae (20-40%) • Splinter hemorrhages (15%) • Osler nodes (10-20%) • Janeway lesions (< 10%) • Splenomegaly 20-50% • Septic complications 20% • Clubbing 10-50% Adapted from Mandell et al 2000 (Karmpaliotis) and Leder Echo Conference 2007
Splinter hemorrhages Under fingernails Usually linear & red Conjunctival petechiae Osler’s nodes (ouch!) Tender SQ nodules Pulp of digits/thenar eminence Janeway lesions Nontender, erythematous, hemorrhagic, or pustular, often on the palms/soles Common Peripheral Manifestations of IE .Reference:Firsche,C. and others,Mitral-Valve Endocarditis,N Engl J Med.Vol. 345,NO.10,September6,2001,P739.
Cardiac Complications • CHF • 2° infection-induced valvular damage (AoV > MV) • MI • 2° embolism of vegetation fragments → CHF • Pericarditis • 2° coronary artery embolization → MI → pericarditis • Extension beyond valve annulus • ↑ CHF, need for cardiac surgery, death • Extension into septum • AV, fascicular, or BBB • Erosion of mycotic aneurysm of sinus of Valsalva • Pericarditis, hemopericardium/tamponade, fistulas to R or L ventricle
Clinical Laboratory (+) blood cultures Non-specific findings Anemia Leukocytosis Abnormal UA ↑’ed ESR & CRP Electrocardiographic New AV block Moderately high PPV for formation of myocardial abscess, but sensitivity low New fascicular block New BBB Suggestive of perivalvular invasion, particularly if AV IE Echocardiographic Diagnosis
Diagnosis • Duke criteria (clinical + laboratory + ECHO) • High specificity 99% • NPV > 92% • Retrospective study 410 patients with IE • 72-90% agreement with ID expert assessment • Most discrepencies 2º overly broad categorization of “possible” IE (experts rejected) • Gave rise to “Modified Duke Criteria”
Modified Duke Criteria • Definite • 2 major • 1 major + 3 minor • 5 minor • Possible • 1 major + 1 minor • 3 minor
Modified Duke Criteria • Major • Evidence of endocardial involvement with new regurgitant murmur • Persistently (+) blood cultures • ECHO • Discrete, echogenic, oscillating intracardiac mass located at site of endocardial injury • Periannular abscess • New dehiscence of a prosthetic valve
Modified Duke Criteria • Minor • Predisposition to IE (certain cardiac conditions/IVDU) • High risk • Prior IE • AoV • RHD • Prosthetic valve • Coarctation • Complex cyanotic congenital heart disease • Moderate risk • MVP with MR +/- thickened leaflets • Isolated MS • Tricuspid valve disease • PS • HCM • Low or no-risk • Secundum ASD • Ischemic heart disease • CABG • MVP without MR and thickened leaflets
Modified Duke Criteria • Minor • Fever > 38° C • Vascular phenomenon • Aside from petechiae & splinter hemorrhages • Immunologic phenomena • RF • GN • Osler’s nodes • Roth spots • Microbiologic findings • (+) blood cultures that do not meet the major criteria
Transthoracic – rapid, non-invasive ↑ Specificity 98% Sensitivity 60-70% Challenging 2° obesity, COPD, chest wall deformities Transesophageal – more costly, invasive Sensitivity 75-95% Specificity 85-98% NPV > 92% Particularly useful if: Prosthetic valves Evaluation of myocardial invasion Diagnosis - Echocardiography
Echocardiography - Indications • Pre-test probability of IE < 4% • TTE both cost effective & satisfactory for r/o IE • Probability of IE 4-60% • TEE initially more cost effective, diagnostically efficient • Unexplained bacteremia with GPC’s • Catheter-associated S. aureus bacteremia • Fever or persistent bacteremia with IVDU
TEE > TTE • Signs of perivalvular extension/presence of myocardial abscess • Fever or persistent bacteremia • Heart block • CHF • New pathologic murmur in patient with IE • Spectral & color-flow Doppler on TEE demonstrate flow • Fistulas • Pseudoaneurysms • Unruptured abscess cavities • Valve perforations
TEE > TTEAoV Regurgitation with Vegetation & Valvular Destruction
AoV Vegetation TEE Echodense mass attached to the noncoronary cusp of the AoV c/w a vegetation using TEE
Mitral Valve Vegetation with Abscess FIGURE 1. Mitral valve vegetation shown on transesophageal echocardiography. The echodense area at the annulus (arrow) is characteristic of underlying abscess.
Multiple Vegetations AoV and MV TTE PLA during diastole. Multiple vegetations on the anterior leaflet of the patient's mitral valve (arrows 1 and 2) and a 16 × 6 mm mobile vegetation on the aortic noncoronary cusp (arrow 3)
M Mode TTE MV with Multiple Echoes from Vegetations M-mode echocardiogram demonstrating multiple echoes from vegetations on the anterior leaflet of the MV during diastole. Specific sign of cusp vegetations in IE.
Aspergillus Prosthetic Valve Endocarditis Causing Functional AS Transesophageal echocardiography (TEE) was performed and revealed a 4 x 2 cm mass on the bioprosthetic AoV, encasing all three leaflets and severely limiting leaflet excursion (Figure 2). Doppler examination revealed a peakgradientof nearly 100 mmHg.
IV antimicrobial therapy for 4-6 weeks Dependent upon pathogen Native vs prosthetic valve PCN G +/- gentamicin Nafcillin/oxacillin +/- gentamicin Vancomycin +/- gentamicin Ceftriaxone Treatment
Anticoagulation Has not been shown to prevent embolization May ↑ risk of intracerebral hemorrhage S. aureus prosthetic valve IE particularly susceptible Role of aspirin still under investigation Treatment
Surgical Therapy for Native Valve IE: Class I Indication (All < LOE B) • Valvular stenosis or regurgitation → CHF • Strongest indication • Mortality in med rx 56-86% vs 11-35% med rx/surgery • Hemodynamics @ time of surgery principle determinant of operative mortality • AR or MR with hemodynamic e/o: • ↑’ed LVEDP • ↑’ed LA pressures • Moderate to severe pulmonary artery systolic HTN • IE 2° fungal or other highly resistant organisms • Pseudomonas, brucella, coxiella, candida, ?enterococci (no synergistic Rx) • lE complicated by: • Heart block • Annular or aortic abscess • Destructive penetrating lesions • Sinus of Valsalva to RA, RV, LA fistula • Mitral leaflet perforation with AoV endocarditis • Infection in annulus fibrosa
Surgical Therapy for Native Valve IE: Other Indications (Both LOE C) • Class IIa • Recurrent emboli & vegetations despite ABX • Class IIb • Mobile vegetations > 10 mm with or without emboli
Surgical Therapy for Prosthetic Valve IE: Class I Indication (All LOE < B) • Consultation with a cardiac surgeon • Heart failure • Dehiscence via cine-fluoroscopy or ECHO • ↑ obstruction or regurgitation • Complications (e.g. abscess formation)
Surgical Therapy for Prosthetic Valve IE: Other Indications (All LOE C) • Class IIa • Persistent bacteremia/recurrent emboli despite ABX • If cerebral infarcts, risk of worsening neurological deficits dependent upon time from initial embolus until surgery • < 7 days, 8-14 days, > 4 weeks (44%, 16.7%, 2.3%) • Relapsing infection • Class III • Not indicated if uncomplicated IE 2° 1st time infection with a sensitive organism
Mortality Rates • Vary according to: • Causative microorganism • > 50 % pseudomonas • 25-47% S. aureus • 15-25% enterococci • 5-37% Q-fever • 4-16% Strep viridans • Presence of complications or coexisting conditions • CHF, neuro events, renal failure, severe immunosuppression 2° HIV • Development of perivalvular extension/myocardial abscess • Use of combined medical and surgical Rx in appropriate patients • Death 2° CNS embolic events/hemodynamic deterioration • Native-valve/prosthetic valve as high as 20-25% • R-sided IE in IVDU approximately 10%
Relapse Rates • Usually occurs within 2 months of DC’ing ABX • Native valve • PCN-sensitive strep viridans < 2% • Enterococcus 8-20% • S. aureus, enterobacter, fungi • Rx failure during 1° course of ABX • Prosthetic valve • 10-15% • (+) blood culture at time of valve replacement RF for relapse, particularly if staphylococcus endocarditis
Procedures That May Result in Transient Bacteremia • Dental • Manipulation of gingival tissue or periapical region of teeth • Respiratory tract • Incision or biopsy of respiratory tract mucosa (e.g. tonisillectomy, bronchoscopy with biopsy) • GI/GU tract • No longer considered high risk – no prophylaxis, unless active GI/GU infection • Skin/Musculoskeletal tissue • If polymicrobial infection undergoing a surgical procedure • Pregnancy • Only in highest risk cardiac conditions undergoing vaginal delivery
Indications for Antibiotic Prophylaxis • Prior history of IE • Prosthetic heart valves (including bioprosthetic & homograft) • Unrepaired cyanotic congenital heart disease • Including palliative shunts and conduits • Completely repaired congenital heart defects with prosthetic material or device, whether placed by surgery or by catheter intervention during the 1st 6 months after the procedure • Repaired congenital heart disease with residual defects at or adjacent to the site of the prosthetic device • Cardiac valvulopathy in a transplanted heart
Antibiotic Prophylaxis No Longer Needed • Bicuspid AoV • Acquired aortic or mitral valve disease including: • MVP with regurgitation • Prior valve repair • HCM with latent or resting obstruction






















