Download

1 / 31
330 likes | 767 Views
Alopeia areata. BY: MOHAMMED ALSAIDAN. Alopecia areata. Alopecia areata affects all age groups and different ethnicities , with equal sex distribution occur in 0.1% to 0.2 % of the general population. Clinical features .

E N D
Alopeiaareata BY: MOHAMMED ALSAIDAN
Alopecia areata • Alopecia areata affects all age groups and different ethnicities, with equal sex distribution • occur in 0.1% to 0.2 % of the general population
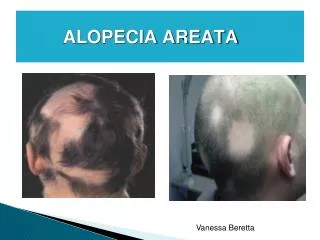
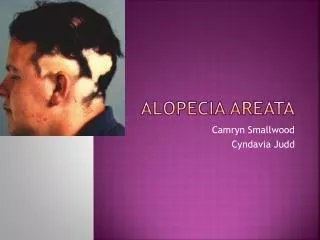
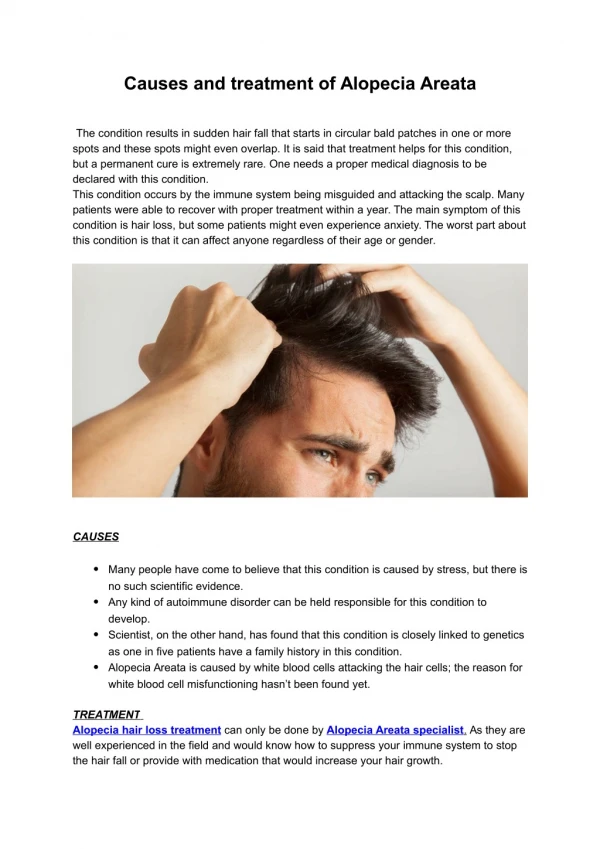
Clinical features • Classic AA lesions are well demarcated, round or oval, completely bald, smooth-surfaced patches • Patches can be mildly reddened or peachy in color • A characteristic finding that is frequently seen in (or at the border of) the patches is ‘‘exclamation mark hairs.’’ • hair pull test may be positive at the periphery of lesions • Initial sparing of white hairs in patients with graying hair
Pattern • ophiasistype, band-like hair loss in parieto-temporo-occipital area • Ophiasisinversus(sisapho), very rare band-like hair loss in the fronto-parieto-temporal area • Reticular patches of hair loss • diffuse thinning over part or all of the scalp. • Acute diffuse and total alopecia: rapid progression and extensive involvement, along with a favorable prognosis
DDx • Trichotillomania and tineacapitis are the most important differential diagnoses in children • Lupus , secondary syphilis and congenital atrichia • diffuse AA can be easily misdiagnosed as telogen effluvium
Prognosis • the most important prognostic factor is the extent of AA involvement or oran ophiasis pattern • Other factors: long duration , atopy, a positive family history, other autoimmune diseases, nail involvement, and young age of first onset • Approximately 5% of cases will progress to AT/AU. • In AT/AU, the chance of full recovery is less than 10% • Up to 50% of patients will recover within 1 year even without treatment
Associations • AA can be associated with nail changes in as many as 66% of patients • Autoimmune diseases, particularly thyroiditis, are the most significant association (8% and 28%) • Other associations include vitiligo, atopy, down syndrome, psychiatric and asymptomatic ophthalmologic changes 41% • IDDM ?
Labs • Routine testing is not indicated in AA • Potassium hydroxide, fungal culture, lupus serology, syphilitic screening, and a scalp biopsy may be necessary
Pathology • A peribulbar lymphocytic infiltrate ‘‘swarm of bees’’ characterizes the acute phase of AA • In subacute cases, large numbers of catagen and telogen hairs will be present • Hair follicle miniaturization with minimal or no inflammation is seen in chronic cases
Treatment : INTRALESIONAL CORTICOSTEROIDS • Intralesional corticosteroids are the treatment of choice for adults • The authors’ preference is triamcinolone acetonide 5mg/mL to the scalp and 2.5mg/mL to the face every 4 to 6 weeks • Treatment should be stopped if there is no improvement after 6 months
Treatment : TOPICAL CORTICOSTEROIDS • Topical midpotentcorticosteroids are the treatment of choice in children • The authors combine topical corticosteroids with minoxidil 5% • Minoxidil5% is mainly used as adjuvant treatment to conventional therapy
Treatment : Anthralin • Anthralin0.5% to 1% short contact therapy is used as alternative treatment • Mild irritation should develop in order for it to work • Anthralinshould not be combined with corticosteroids • Treatment may be stopped if there is no improvement after 3 months
Treatment : TOPICAL IMMUNOTHERAPY • Diphenylcyclopropenone(DPCP) is the treatment of choice for adults with more than 50% scalp involvement • Sensitization with DPCP 2% is followed by weekly application of the lowest concentration that can cause mild irritation • Treatment should be stopped if there is no improvement after 6 months • Squaricacid dibutylester is an alternative in patients who do not develop allergic reaction to DPCP (DNCP: MUTAGENIC) • The success rate is 50% to 60%, with a relapse rate up to 62% at a median period of 2 and a half years
Initially, 2% DPCP in acetone is applied to a 4- 4-cm circular area of the scalp Two weeks later, a 0.001% DPCP solution is applied to the same half of the scalp The concentration of DPCP is increased gradually each week until a mild dermatitis reaction is obtained. The goal is to achieve a low-grade erythema and mild pruritus DPCP should be left on the scalp for 48 hours, with sun avoidance Lag for evident clinical improvement 3-12 month
Treatment : Capsaicin • Capsaicin was previously shown to induce vellus hair regrowth in AA • More recently, a study showed that topical capsaicin and clobetasol 0.05% are comparable Bexarotene • In a single recently published study, bexarotene 1% gel resulted in a 26% hair regrowth rate • Dermal irritation is a common side effect Topical calcineurin inhibitors • failed to show hair regrowth in AA
Treatment : Systemic corticosteroids • Daily, weekly, and monthly pulse corticosteroids have been used with varying success • The use of systemic corticosteroids is limited by their side effect profile and a higher rate of relapse
Treatment : Cyclosporine • Cyclosporine has been used alone or in conjunction • with corticosteroids with a success rate up to 76.6% • Cyclosporine use is limited by its side effects and high relapse rate
Treatment : Sulfasalazine • Sulfasalazine up to 1.5 g twice daily is successful in about quarter of the patients • The relapse rate is 45.5% • One in three patients may have side effects
Treatment : Methotrexate • Methotrexate in conjunction with low-dose prednisone showed success in 64% of patients with AT/AU in one study Biologics • Several reports of multiple biologics, including etanercept, efalizumab, adalimumab, and infliximab failed to show improvement in AA
Treatment : Photochemotherapy • Systemic and topical psoralen plus ultraviolet A light phototherapy have been used with limited success • Long-term safety, side effects, and a high relapse rate have curtailed the use of psoralen plus ultraviolet A light phototherapy
Treatment : Other phototherapies • Excimerlaser may be helpful in limited patchy AA • Infrared irradiation as monotherapy or adjunctive to conventional therapy showed some success
Treatment : Psychological support
Pathophysiology • AA is a lymphocyte cell mediated inflammatory form of hair loss with underlying autoimmune etiopathogenesis • dystrophic anagen hair follicles and/or increased frequency of telogenstate follicles • Genetic susceptibility to the development of AA involves specific alleles of the HLA region though other non-HLA genes are also likely to be involved • Susceptibility to the development of AA may be modified by environmental factors, including exposure to proinflammatoryagents and possibly other modulators, including stress and diet