Download
1 / 102
1.04k likes | 1.7k Views
Colon, Anus, Rectum. Random animal/human evacuating bowels. Embryology and Anatomy. Embryology Starts the fourth week of gestation derived from the endoderm three segments: foregut, midgut, and hindgut midgut and hindgut contribute to the colon, rectum, and anus

E N D
Embryology and Anatomy • Embryology • Starts the fourth week of gestation • derived from the endoderm • three segments: foregut, midgut, and hindgut • midgut and hindgut contribute to the colon, rectum, and anus • Hindgut - distal transverse colon, descending colon, rectum, and proximal anus all blood supply from IMA • Anatomy • anatomically and functionally divided into the colon, rectum, and anal canal • five distinct layers: mucosa, submucosa, inner circular muscle, outer longitudinal muscle (tenea coli), and serosa (not present in mid and lower rectum)
Colon • Terminal ileum 3 to 5 ft to the rectum • Rectosigmoid junction (level of the sacral promontory) point at which the three teniae coli coalesce • Cecum is the widest diameter (normally 7.5 to 8.5 cm) and thinnest muscular wall (set up to perf) • Sigmoid colon has a narrow caliber, making it the most vulnerable to obstruction
Arterial Supply • SMA - • Ileocolic artery (absent in up to 20% of people), terminal ileum and proximal ascending colon • Right colic artery - ascending colon • Middle colic artery - transverse colon • IMA - • Left colic artery - descending colon • Sigmoidal branches - sigmoid colon • Superior rectal artery - proximal rectum • Communicate via the marginal artery of Drummond, complete in only 15 to 20% of people
Veins, Lymphatics, and Innervation Veins • Veins of the colon parallel their corresponding arteries (except IMV) and bear the same terminology • Inferior mesenteric vein ascends in the retroperitoneal plane over the psoas muscle, posterior to the pancreas to join the splenic vein. (During a colectomy, mobilized independently and ligated at the inferior edge of the pancreas) Lymphatic Drainage • Muscularis mucosa -> follow the regional arteries. Lymph nodes are found on the bowel wall (epicolic), along the inner margin of the bowel adjacent to the arterial arcades (paracolic), around the named mesenteric vessels (intermediate), and at the origin of the superior and inferior mesenteric arteries (main). Nerve Supply • Sympathetic (inhibitory) and parasympathetic (stimulatory) nerves, which parallel the course of the arteries. Sympathetic nerves arise from T6–T12 and L1–L3. Vagus nerve ->parasympathetic innervation to the right and transverse colon; parasympathetic nerves to the left colon arise from sacral nerves S2–S4 to form the nervi erigentes.
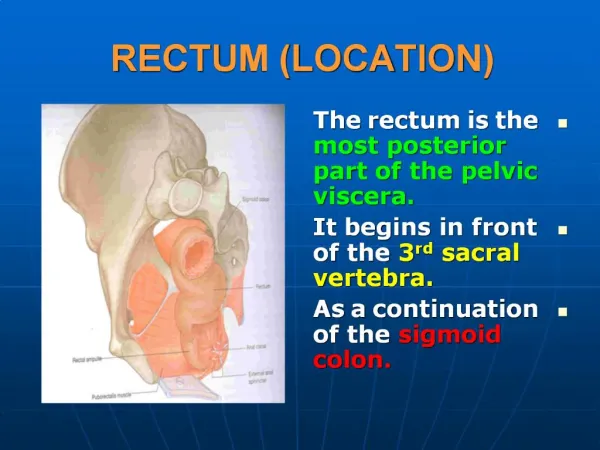
Anorectal • Rectum -12 to 15 cm in length • Valves of Houston - three distinct submucosal folds • Posteriorly -presacral fascia, • Anteriorly - Denonvilliers' fascia • Lateral ligaments support the lower rectum • Surgical anal canal measures 2 to 4 cm (anorectal junction to anal verge) • Dentate or pectinate line transition columnar rectal mucosa and squamous anoderm, surrounded by longitudinal mucosal folds, known as the columns of Morgagni, (anal crypts empty here, source of cryptoglandular abscesses) • Inner smooth muscle is thickened and comprises the internal anal sphincter • Deep external anal sphincter is an extension of the puborectalis muscle • Puborectalis, iliococcygeus, and pubococcygeusmuscles form the levator ani muscle
Anorectal Vascular Supply • Superior rectal artery <- inferior mesenteric artery (upper rectum) • Middle rectal artery <- internal iliac • Inferior rectal artery <- internal pudendal <- internal iliac artery. • Rich collaterals
Veins and Lymphatics Venous • Superior rectal vein -> inferior mesenteric -> portal system • Middle rectal vein -> internal iliac vein • Inferior rectal vein -> internal pudendal vein -> internal iliac vein • Submucosal plexus deep to the columns of Morgagni forms the hemorrhoidal plexus and drains into all three veins. Anorectal Lymphatic Drainage • Parallels the vascular supply • Upper and middle rectum -> inferior mesenteric nodes • Lower rectum -> inferior mesenteric and internal iliac nodes Anal canal • Proximal to the dentate line -> inferior mesenteric and internal iliac nodes • Distal -> inguinal nodes, inferior mesenteric and internal iliac nodes
Anorectal Nerve Supply • Sympathetic - L1–L3 -> preaortic plexus -> hypogastric plexus combine with -> • Parasympathetic (nervi erigentes) S2–S4 to form the pelvic plexus. • Sympathetic and parasympathetic fibers then supply the anorectum and adjacent urogenital organs. • The internal anal sphincter is innervated by sympathetic and parasympathetic nerve fibers; both inhibit sphincter contraction. • The external anal sphincter and puborectalis muscles are innervated by the inferior rectal branch of the internal pudendal nerve.
Normal Physiology Fluid and Electrolyte Exchanges • The colon is a major site for water absorption and electrolyte exchange. • 90% of the water contained in ileal fluid is absorbed in the colon (1000 to 2000 mL/d), and up to 5000 mL of fluid can be absorbed daily • Sodium is absorbed actively via a Na-K ATPase. The colon can absorb up to 400 mEq of sodium per day. • Water accompanies the transported sodium and is absorbed passively along an osmotic gradient. • Potassium is actively secreted • Chloride is absorbed actively via a chloride–bicarbonate exchange. • Bacterial degradation of protein and urea produces ammonia. Ammonia is subsequently absorbed and transported to the liver.
Colonic Microflora and Intestinal Gas • Approximately 30% of fecal dry weight is composed of bacteria (1011 to 102 bacteria/g of feces). • Anaerobes predominant • Bacteroides species are the most common (1011 to 1012 organisms/mL) > Escherichia coli are the most numerous aerobes (108 to 1010 organisms/mL). Breakdown of carbs, bilirubin, etc. • Short-chain fatty acids (acetate, butyrate, and propionate) are produced by bacterial fermentation of dietary carbohydrates, lack may result in mucosal atrophy and "diversion colitis." • Produce vitamin K. • Hold off Clostridium difficile and other invaders • Intestinal gas arises from swallowed air, diffusion from the blood, and intraluminal production.
Motility • No cyclic motor activity characteristic of the migratory motor complex. Instead, the colon displays intermittent contractions of either low (delay colonic transit) or high amplitude (move contents). Defecation • Distention of the rectum causes a reflex relaxation of the internal anal sphincter (the rectoanal inhibitory reflex) that allows the contents to make contact with the anal canal. This "sampling reflex" allows the sensory epithelium to distinguish solid stool from liquid stool and gas. • Coordination of increasing intra-abdominal pressure via the Valsalva maneuver, increased rectal contraction, relaxation of the puborectalis muscle, and opening of the anal canal. Continence • At rest, the puborectalis muscle creates a "sling" around the distal rectum, forming a relatively acute angle that distributes intra-abdominal forces onto the pelvic floor. With defecation, this angle straightens, allowing downward force to be applied along the axis of the rectum and anal canal. • Internal sphincter is responsible for most of the resting, involuntary sphincter tone (resting pressure). • External sphincter is responsible for most of the voluntary sphincter tone (squeeze pressure). • Branches of the pudendal nerve innervate both the internal and external sphincter.
Tools of the Trade Anoscopy • Anal canal. • 8cm but variable • Anal procedures such as rubber band ligation or sclerotherapy of hemorrhoids Proctoscopy • Rectum and distal sigmoid colon • 25 cm in length. • Polypectomy, electrocoagulation, or detorsion of a sigmoid volvulus Flexible Sigmoidoscopy • Colon and rectum (to splenic flexure) • 60 cm in length Colonoscopes • 100 to 160 cm in length • Entire colon and terminal ileum • Bowel preparation, conscious sedation Capsule Endoscopy • Images transmitted by radiofrequency • Primarily small bowel lesions
Imaging Plain X-Rays and Contrast Studies • Free intra-abdominal air, bowel gas patterns suggestive of small or large bowel obstruction, and volvulus. • Contrast studies are useful for evaluating obstructive symptoms, delineating fistulous tracts, and diagnosing small perforations or anastomotic leaks. • Gastrografin –less detail, water soluble, use if perforation • Double-contrast barium enema 70 to 90% sensitive for the detection of mass lesions greater than 1 cm in diameter. (back-up examination if colonoscopy is incomplete) Computed Tomography • Good for extraluminal disease • Perforation or anastomotic leak, nonspecific findings such as bowel wall thickening or mesenteric stranding may suggest inflammatory bowel disease, enteritis/colitis, or ischemia.. • Not good for intraluminal pathology Virtual Colonoscopy/Computed Tomography Colography • Helical CT and three-dimensional reconstruction to detect intraluminal colonic lesions. Oral bowel preparation, oral and rectal contrast, and colon insufflation • Approaches colonoscopy’s sensitivity Magnetic Resonance Imaging • Detecting bony involvement or pelvic sidewall extension of rectal tumors, determines the extent of spread of rectal cancer into adjacent structures • Detection and delineation of complex fistulas in ano
Imaging Positron Emission Tomography • Imaging tissues with high levels of anaerobic glycolysis (malignant tumors) • F-fluorodeoxyglucose • Adjunct to CT in the staging of colorectal Angiography • Detection of bleeding within the colon or small bowel. • Must be relatively brisk (approximately 0.5 to 1.0 mL per minute) • If identified, infusion of vasopressin or angiographic embolization can be therapeutic. Endorectal Ultrasound • Evaluate the depth of invasion of neoplastic lesions in the rectum. • Can detect enlarged perirectal lymph nodes
Laboratory Studies Fecal Occult Blood Testing • Screening test for colonic neoplasms in asymptomatic, average-risk individuals. • Serial testing, colorectal malignancies will bleed intermittently • Red meat, some fruits and vegetables, and vitamin C will produce a false-positive result • Any positive FOBT mandates further investigation, usually by colonoscopy. Stool Studies • Stool studies often are helpful in evaluating the etiology of diarrhea. • Wet-mount - fecal leukocytes <- colonic inflammation or the presence of an invasive organism such as invasive E. coli or Shigella. • Stool cultures can detect pathogenic bacteria, ova, and parasites. • C. difficile colitis is diagnosed by detecting bacterial toxin or PCR • Steatorrhea may be diagnosed by adding Sudan red stain to a stool sample.
Tumor Markers • Carcinoembryonic antigen (CEA) 60 to 90% with colorectal cancer • Not an effective screening tool • Follow to detect early recurrence of colorectal cancer • No survival benefit has yet been proven.
Pain!!!!!!!!!! Abdominal pain • Differential: obstruction (either inflammatory or neoplastic), inflammation, perforation, or ischemia. • Plain x-rays and judicious use of contrast studies and/or a CT • Gentle retrograde contrast studies (barium or Gastrografin enema) sigmoidoscopy and/or colonoscopy (ischemic colitis, infectious colitis, and inflammatory bowel disease) Pelvic pain • Distal colon and rectum or from adjacent urogenital structures. • Tenesmus may result from proctitis or from a rectal or retrorectal mass. • Cyclical pain associated with menses= endometriosis. • Pelvic inflammatory peridiverticular abscess or periappendiceal abscess into the pelvis may also cause pain. • CT scan and/or MRI, proctoscopy, laparoscopy Anorectal pain • Most often anal fissure, perirectal abscess and/or fistula, or a thrombosed hemorrhoid >> anal canal neoplasms, perianal skin infection. • Proctalgia fugax results from levator spasm • Physical examination is key, (DRE)
Lower Gastrointestinal Bleeding • ABCs and adequate resuscitation. • Correct coagulopathy and/or thrombocytopenia • Most common source of GI hemorrhage is upper GI: esophageal, gastric, or duodenal, so nasogastric aspiration should always be performed • Not negative unless return of bile suggests that the source of bleeding is distal to the ligament of Treitz. • EGD if not negative • Anoscopy and/or limited proctoscopy for hemorrhoidal bleeding. • Technetium-99–tagged red blood cell scan is extremely sensitive and is able to detect as little as 0.1 mL/h of bleeding but imprecise. • Angiography, vasopressin or angioembolization may be therapeutic, catheter can be left in the bleeding vessel to allow localization at the time of laparotomy. • Colonoscopy if stable, cautery or injection of epinephrine • Colectomy may be required if bleeding persists, segmental resection is preferred if the bleeding source can be localized. • "Blind" subtotal colectomy may very rarely be required, must r/o rectal source
Occult Blood Loss • Presents as iron-deficiency anemia or + FOBT, if positive do colonoscopy • Neoplasms bleed intermittently • Hematochezia -> hemorrhoids (painless (internal), bright-red rectal bleeding with bowel movements) or fissure (sharp, knife-like pain and bright-red rectal bleeding with bowel movements) • Digital rectal examination, anoscopy, and proctosigmoidoscopy, if nothing found, do colonoscopy.
Constipation and Obstructed Defecation • Extremely common (4 million in U.S.A.) • Metabolic, pharmacologic, endocrine, psychological, and neurologic contribute • Exclude stricture or mass lesion by colonoscopy or barium enema • Evaluation focuses on differentiating slow-transit constipation (radiopaque markers) from outlet obstruction (anorectal manometry and EMG of the puborectalis) • Defecography can identify rectal prolapse, intussusception, rectocele, or enterocele. • Medical management is the mainstay: fiber, increased fluid intake, and laxatives • Outlet obstruction -> biofeedback • Subtotal colectomy is considered only for patients with severe slow-transit constipation (colonic inertia) refractory to maximal medical interventions -> complaints of diarrhea, incontinence, and abdominal pain.
Diarrhea • Further investigation is warranted if diarrhea is chronic or is accompanied by bleeding (colitis) or abdominal pain • Infection (invasive E. coli, Shigella, Salmonella, Campylobacter, Entamoeba histolytica, or C. difficile) ->stool wet-mount and culture • Inflammatory bowel disease (ulcerative colitis or Crohn's colitis) -> scope • Ischemia -> scope (if stable)
Chronic diarrhea • Chronic ulcerative colitis, Crohn's colitis, infection, malabsorption, and short-gut syndrome can cause chronic diarrhea. • Carcinoid syndrome and islet cell tumors (VIP, somatostatinoma, gastrinoma), large villous lesions • Biopsies should be taken even if the colonic mucosa appears grossly normal.
Irritable bowel syndrome • Crampy abdominal pain, bloating, constipation, and urgent diarrhea. • No underlying anatomic or physiologic abnormality. • Diagnosis of exclusion • Dietary restrictions and avoidance of caffeine, alcohol, and tobacco may help to alleviate symptoms. • Antispasmodics and bulking agents may help
Emergency Resection • Obstruction, perforation, or hemorrhage. • Bowel is almost always unprepared and the patient may be unstable. • Attempt should be made to resect the involved segment along with its lymphovascular supply. • Right colon or proximal transverse colon, a primary ileocolonic anastomosis usually can be performed safely as long as the remaining bowel appears healthy and the patient is stable. • Left-sided tumors-resection and end colostomy, with or without a mucus fistula. • Increasing data for primary anastomosis without a bowel preparation or with an on-table lavage, w/w/o diverting ileostomy, may be equally safe in this setting. • Subtotal colectomy with a small bowel to rectosigmoid anastomosis if the proximal colon looks unhealthy • Resection and diversion (ileostomy or colostomy) remains safe and appropriate if the bowel looks compromised or if the patient is unstable, malnourished, or immunosuppressed
Minimally Invasive Techniques of Resection • Laparoscopically or with hand-assisted laparoscopy. • Improved cosmetic result, decreased postoperative pain, earlier return of bowel function, and possible decrease in immunosuppressive impact • Most studies have demonstrated equivalence between laparoscopic and open resection in terms of extent of resection. • Pequire longer operative time than do open procedures. • Return of bowel function and length of hospital stay are highly variable, but appear to be better.
Procedures Ileocolic Resection • Resection of terminal ileum, cecum, and appendix • Benign lesions or incurable cancers arising in the terminal ileum, cecum, and, occasionally, the appendix • Ileocolic vessels are ligated and divided. • Primary anastomosis distal small bowel to ascending colon • Most distal ileum needs to be resected Right Colectomy • Most appropriate operation for curative intent resection of proximal colon carcinoma. • Ileocolic vessels, right colic vessels, and right branches of the middle colic 10 cm of terminal ileum included • Ileal-transverse colon anastomosis • Extended right colectomy for curative for lesions at the hepatic flexure or proximal transverse colon Transverse Colectomy • Ligating the middle colic vessels • Colocolonic anastomosis • Extended right colectomy safer
Procedures Left Colectomy • For lesions in distal transverse colon, splenic flexure, or descending colon • Left branches of the middle colic vessels, the left colic vessels, and the first branches of the sigmoid vessels are ligated. • Colocolonic anastomosis usually can be performed. Sigmoid Colectomy • Divide sigmoid branches of the inferior mesenteric artery • Entire sigmoid colon should be resected to the level of the peritoneal reflection • Descending colon to upper rectum • Full mobilization of the splenic flexure for tension-free anastomosis Total and Subtotal Colectomy • Fulminant colitis, attenuated FAP (AFAP), or synchronous colon carcinomas • Divide ileocolic vessels, right colic vessels, middle colic vessels, and left colic vessels leave superior rectal vessels • Subtotal colectomy with ileosigmoid anastomosis – distal sigmoid left • Sigmoid completely removed- total abdominal colectomy with ileorectal anastomosis • End-ileostomy - remaining sigmoid or rectum made into mucus fistula or Hartmann pouch. Total Proctocolectomy • Colon, rectum, and anus are removed and the ileum is brought to the skin as a Brooke ileostomy. • Restorative Proctocolectomy (Ileal Pouch Anal Anastomosis) • Colon and rectum resected, but the anal sphincter muscles portion of the distal anal canal are preserved.
Procedures High Anterior Resection • Distal sigmoid colon and upper rectum for benign lesions and disease at the rectosigmoid junction such as diverticulitis. • Primary anastomosis (usually end-to-end) between the colon and rectal stump with a short cuff of peritoneum surrounding its anterior two thirds Low Anterior Resection • Lesions in the upper and midrectum. • The rectosigmoid is mobilized, the pelvic peritoneum is opened • Dissection to the anorectal ring • Requires mobilization of the splenic flexure Extended Low Anterior Resection • For distal rectum lesions but several centimeters above the sphincter • Coloanal anastomosis • Creation of a temporary ileostomy • Can create colon J-pouch if no sphincter damage
Procedures Hartmann's Procedure and Mucus Fistula • colostomy or ileostomy is created and the distal colon or rectum is left as a blind pouch • mucus fistula if enough bowel present Abdominoperineal Resection • entire rectum, anal canal, and anus with construction of a permanent colostomy from the descending or sigmoid colon • Anastomoses • end-to-end (roughly the same caliber), end-to-side (one limb of bowel is larger than the other), side-to-end (proximal bowel is of smaller caliber than the distal bowel, ileorectal), or side-to-side (ileocolic and small bowel anastomoses) • handsewn (single or double layer(continuous inner layer and an interrupted outer layer)) or stapled (particularly useful for creating low rectal or anal canal anastomoses) • none has been proven to be superior • submucosal layer of the intestine provides the strength of the bowel wall • NO tension in a normotensive • Highest risk - distal rectal or anal canal, involve irradiated or diseased intestine, or are performed in malnourished, ill patients.
Ostomies • Temporary or permanent, end-on or a loop • Placement and construction are crucial for function • Located within the rectus muscle to minimize the risk of a postoperative parastomal hernia • Must be in plain sight • Preoperative evaluation by ostomy nurse (sight and teaching)
More Ostomy Temporary Ileostomy - loop ileostomy • Subsequent closure often can be accomplished without a formal laparotomy • Flexible endoscopy exam and a contrast enema (Gastrografin) are recommended before closure Permanent Ileostomy • After total proctocolectomy or in patients with obstruction. • End ileostomy is the preferred configuration • Stitches often are used to secure the bowel to the posterior fascia. Complications of Ileostomy • Stoma necrosis - skeletonizing or tight fascial defect • Necrosis below the level of the fascia requires surgical revision • Stoma retraction may occur early or late • Dehydration fluid and electrolyte abnormalities, keep at less than 1500 mL/d • Bulk agents and opioids (Lomotil, Imodium, tincture of opium) are useful. Obstruction • Parastomal hernia - symptomatic should be repaired, re-siting the stoma to the contralateral side of the abdomen. • Prolapse (rare)
Colostomy • Most end colostomies >> loop colostomies (too bulky and prolapse is more likely) • Should be matured in a Brooke fashion • Mucus fistula or Hartmann's pouch • Closure generally requires laparotomy Complications of Colostomy • Necrosis management similar to ileostomy • Retraction less problematic with a colostomy • Obstruction is unusual • Parastomal hernia is the most common late complication of a colostomy (repair if it is symptomatic) • Prolapse occurs rarely • Dehydration is rare Functional Results • Usually excellent • Uncommon diarrhea and bowel frequency.
Positioning • Most abdominal colectomies can be performed in the supine position. Anterior and APRs require lithotomy positioning. Bowel Preparation • Decreasing the bacterial load in the colon and rectum (not proven) • Most commonly used regimens include polyethylene glycol (PEG) solutions or sodium phosphate, equally efficacious in bowel cleansing. • Oral antibiotics to decreasing the bacterial load of the colon. never been proven to decrease postoperative infectious complications. • Ideally, a stoma should be placed in a location that the patient can easily see and manipulate, within the rectus muscle, and below the belt line (see Fig. 29-15). In emergencies, placement high on the abdominal wall is preferred to a low-lying site. Ureteral Stents • Useful for identifying the ureters intraoperatively • Invaluable in reoperative pelvic surgery or when there is significant retroperitoneal inflammation • Lighted stents may be helpful in laparoscopic resections
Inflammatory Bowel Disease Epidemiology • Ulcerative colitis to 15 people per 100,000 • Crohn's disease is slightly lower, one to five people per 100,000 population. Both have bimodal incidence, 15 to 30 years and ages 55 to 60 years. • 15% indeterminate colitis. Etiology • none are proven. • Family history 10 to 30% have a family member with the same disease • Autoimmune vs infectious • Pathology and Differential Diagnosis Ulcerative colitis is a mucosal process • mucosa atrophic and friable, crypt abscesses friable, inflammatory pseudopolyps. Proctitis (just rectum) to pancolitis. • does not involve the small intestine, but "backwash ileitis • continuous involvement of the rectum and bloody diarrhea and crampy abdominal pain, tenesmus. Severe abdominal pain and fever = fulminant colitis or toxic megacolon. Dx with colonoscopy and mucosal biopsy. Crohns disease • transmural and can affect any part of the GI tract from mouth to anus. Mucosal ulcerations, noncaseating granulomas Chronic inflammation may ultimately result in fibrosis, strictures, and fistulas in either the colon or small intestine. Colonoscopy deep serpiginous ulcers and a "cobblestone" appearance. Skip lesions and rectal sparing are common. • diarrhea, crampy abdominal pain, and fever. Strictures may produce symptoms of obstruction. Perianal Crohn's disease may present with pain, swelling, and drainage from fistulas or abscesses. Extraintestinal Manifestations • Fatty infiltration of the liver is present in 40 to 50% cirrhosis is found in 2 to 5%. • 40 to 60% with primary sclerosing cholangitis have ulcerative colitis. Biliary carcinoma fromlong standing disease • Arthritis 20 times greater than in the general population. • Sacroiliitis and ankylosing spondylitis are associated with inflammatory bowel disease • Erythema nodosum is seen in 5 to 15% • Women are affected three to four times more frequently than men. Pyoderma gangrenosum is an uncommon but serious. • Up to 10% will develop ocular lesions.
Principles of Nonoperative Management • Ulcerative proctitis and proctosigmoiditis salicylate and/or corticosteroid suppositories and enemas • Salicylates • Sulfasalazine (Azulfidine), 5-ASA, and related compounds are first-line agents in the medical treatment of mild to moderate inflammatory bowel disease. cyclooxygenase and 5-lipoxygenase Antibiotics • Metronidazole possibly helps with Crohn's colitis but Abx reserved for fulminant colitis or toxic megacolon Corticosteroids • Corticosteroids are a key component • 75 to 90% of patients will improve • Failure to wean corticosteroids is a relative indication for surgery. • Corticosteroid enemas provide effective local therapy for proctitis Other Immunosuppressive Agents • Azathioprine and 6-mercaptopurine are antimetabolite drugs ulcerative colitis and Crohn's disease in patients who have failed salicylate therapy or who are dependent upon or refractory to corticosteroids. • Onset of action of these drugs takes 6 to 12 weeks taken with steriods • Cyclosporine interferes with T-cell function. • Not routinely used to treat inflammatory bowel disease, helps with refractory UC and Crohns • Methotrexate is a folate antagonist efficacy of this agent is unproven • Infliximab (Remicade) is a monoclonal antibody against tumor necrosis factor alpha. moderate to severe Crohn's disease Recurrence is common Nutrition • Patients with inflammatory bowel disease often are malnourished. Pain, obstruction, diarrhea inflammatory catabolic state • TPN suggested
Ulcerative Colitis • Characterized by remissions and exacerbations. • Insidious, with minimal bloody stools, or the onset can be abrupt, with severe diarrhea and bleeding, tenesmus, abdominal pain, and fever. • Dx endoscopically with bx, chronic phase better, don’t perf (acute phase) • Rectum invariably involved • Pus and mucus also may be present. • Barium enema "lead pipe" colon • Emergent surgery - hemorrhage, toxic megacolon, or fulminant colitis who fail to respond rapidly to medical therapy. • Fulminant colitis should be treated aggressively with bowel rest, hydration, broad-spectrum antibiotics, and parenteral corticosteroids. No colonoscopy, barium enema, and antidiarrheal agents are contraindicated. Deteriation or failure to improve within 24 to 48 hours mandates surgery. • Elective surgery - intractability despite maximal medical therapy, side effects not tolerated, significant risk of developing colorectal carcinoma. • Risk of malignancy increases with pancolonic disease and the duration of symptoms is approximately 2% after 10 years, 8% after 20 years, and 18% after 30 years. • Long-standing ulcerative colitis undergo colonoscopic surveillance with multiple (40 to 50), random biopsies to identify dysplasia before invasive malignancy develops (flat polyps)
Ulcerative Colitis Annual surveillance after: • 8 years in patients with pancolitis • 15 years in patients with left-sided colitis • dysplasia - should be advised to undergo proctocolectomy • controversy prophylactic proctocolectomy for chronic UC for >10 years Emergent Operation • Fulminant colitis or toxic megacolon • Total abdominal colectomy with end ileostomy>>>total proctocolectomy Elective Operation • Include resection of the rectum • Indeterminate -> abdominal colectomy with ileorectal anastomosis • Total proctocolectomy with end ileostomy has been the "gold standard" for patients with chronic ulcerative colitis. • restorative proctocolectomy with ileal pouch–anal anastomosis has become the procedure of choice
Crohn's Disease • Exacerbations and remissions. • Any portion of the intestinal tract, from mouth to anus, impossible to remove all of the at-risk intestine • Rectal sparing occurs in 40% • Terminal ileum and cecum (ileocolic Crohn's disease) involved 41% • Internal fistulas (require resection of the segment of bowel), chronic strictures (resection or stricturoplasty) • Length of bowel removed should be minimized. • Bowel should be resected to an area with grossly normal margins ONLY • Stoma should be strongly considered in any patient who is hemodynamically unstable, septic, malnourished, or receiving high-dose immunosuppressive therapy and in patients with extensive intra-abdominal contamination. • Ileocolic and Small Bowel Crohn's Disease • Most common indications for surgery are internal fistula or abscess (30 to 38% of patients) and obstruction (35 to 37% of patients). • Drainage of abscess(es) and antibiotics, • Isolated chronic strictures also should be resected. In patients with multiple fibrotic strictures that would require extensive small bowel resection, stricturoplasty is a safe and effective alternative to resection. • Recurrence 50% in 10 yrs
Crohn's colitis (especially pancolitis) carries nearly the same risk for cancer as ulcerative colitis. • Ileal pouch–anal reconstruction is not recommended • perianal disease occurs in 35% of all patients with Crohn's disease • fissure from Crohn's disease is particularly deep more like an ulcer. They often are multiple and located in a lateral position • Treatment of anal and perianal Crohn's disease focuses on alleviation of symptoms. should not do surgery unless forced, risk of creating chronic, nonhealing wounds. • Drain abscesses, mushroom catheters and liberal use of setons, advancement flaps if minimal disease, intractable perianal sepsis requires proctectomy. • Infliximab and others have shown some efficacy in healing chronic fistulas (drain any and all abscesses before starting)
Indeterminate Colitis • 15% of patients with IBD characteristics of both diseases • Indications for surgery are the same, treat like Crohns