Download
1 / 91
1.14k likes | 2.07k Views
IMMUNOHEMATOLOGY By E. Salehi Ph.D. Assistant prof. Department of Immunology. History ABO System Phenotype ABO System Genotype Rh system Other Blood Groups Blood Group detection and incompatibility Hereditary Newborn Disease HDN Blood Transfusion. Karl Landsteiner (1868-1943).

E N D
IMMUNOHEMATOLOGY By E. Salehi Ph.D. Assistant prof. Department of Immunology • History • ABO System Phenotype • ABO System Genotype • Rh system • Other Blood Groups • Blood Group detection and incompatibility • Hereditary Newborn Disease HDN • Blood Transfusion
Karl Landsteiner (1868-1943) • Discovered ABO blood groups, 1900 • Nobel Prize, 1930
Biological Functions of Blood group Systems • Functional Diversity • Transporters/Channels • Transporting Water-Soluble molecules/compounds • Rh, Colton, Diago, Kx, Kidd • Receptors • Biological • Duffy, Knops, Indian • Microbial • MNS, P, Lewis, Duffy, Cromer • Adhesion Molecules • Leuthran, Xg, L-W, Indian • Role in Complement Pathway • Chido/Rodgers, Cromer, Knops • Enzymes • ABO, P, Lewis, H • Structural Proteins • Maintain Shape • MNS, Diago, Gerbich
Type .2 • Type .1 3 *PS = oligosaccharide chain attached to either glycosphingolipid (RBC) or glycoprotein (secretions).
ABO Antigen Genetics LOCATION • The presence or absenceof the ABH antigens on the red blood cell membrane is controlled by the H gene • The presence or absenceof the ABH antigens in secretions is indirectly controlled by the Se genes.
H Antigen The H gene codes for an enzyme that adds a sugar (Fucose) to the terminal sugar of a Precursor Substance (PS*). The biochemical structure below constitutes the H Antigen. (h gene is an amorph.) H gene acts on a Precursor substance(PS)* by adding Fucose *PS = oligosaccharide chain attached to either glycosphingolipid (RBC) or glycoprotein (secretions).
The H antigen is found on the rbc when you have the Hh or HH genotypes but NOT from the hh genotype. The A antigen is found on the rbc when you have the Hh, HH, and A/A,A/O or A/B genotypes. The B antigen is found on the rbc when you have the Hh, HH, and B/B,B/O or A/B genotypes.
ABO Subgroups • ABO subgroups differ in the amount of antigen present on the red blood cell membrane, specifically, they have less - it is quantitative. • Subgroups are the results of less effective enzymes! Not as efficient at converting H antigens to A or B antigens so fewer are present on the rbc. • Subgroups of A are more common than Subgroups of B.
Subgroups of A • The two principle subgroups of A are: • A1 and A2 • Both react strongly with reagent anti-A. • To distinguish A1 from A2 red blood cells test with plant lectin: Dolichos biflorus • Approximately 80% of Group A and Group AB persons red cells are agglutinated by Dolichos biflorus and can be designated A1 and A1B. • The remaining 20% are A2 and A2B.
ABO Subgroups A2 Phenotype • A2 persons produce anti-A1 allo-antibodies (%1-8) • A2B persons produce anit-A1 allo antibodies (%22-35) • Allo-Anti-A1 can cause ABO Discrepancies (How?) and incompatibility in crossmatching. It is not considered clinically significant if it does not react at 37oC.
Number of A antigen • A1=800000 • A2=250000 • A3=35000 • Ax=4800 • Aend=3500 • Am=700
Amount of H Antigenaccording to ABO Blood Group • Blood Group O people have red blood cells rich in H antigen. Why? Neither the A or B genes have converted the H antigens to A or B antigens - just a whole bunch of H! LeastAmount of H Greatest Amount of H O > A2 > B > A2B > A1 > A1B
Formation Of ABO Antigens In Secretions Hh ABO PS2 ABO on Cells H Antigen ABO PS1 ABO in secretions H Antigen Se se
Bombay (Oh) Phenotype • Results from the inheritance of hh genotype • Red blood cells lack H, A and B antigens • First discovered in Bombay, India • Red cells are NOT agglutinated with anti-A, Anti-B or Anti-H (Ulex europaeus - lectin) • Serum has strong anti-A, Anti-B and anti-H so they agglutinate ALL ABO blood groups ParaBombay (Ah) Phenotype
Ab titer 3-6 mo 5-10 yr A Mystery….Why “preformed” ?
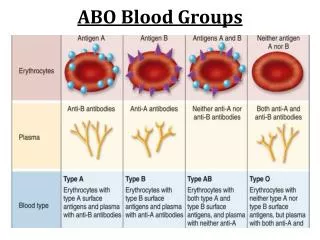
ABO Blood Grouping Reagents • Forward Grouping • Reagent Anti-A and Anti-B • IgM class Monoclonal antibody reagent • Reverse Grouping • Reagent A1 and B cells (3-5% suspension) • Routine tests on donors and patients must include both the forward and reverse grouping
Frequency of ABO Blood Groups • Group O 47% • Group A 42% • Group B 8% • Group AB 3%
The Rh Blood Group System • Described by Landsteiner in 1940 • Antibodies produced as a result of pregnancy or transfusion • Immune antibodies - IgG • Can cause haemolytic disease of the newborn and transfusion reactions
Inheritance of Rh genes • Fisher-Race theory of inheritance • Rh antigens produced by three closely linked alleles C or c, D or d, E or e. (these alleles are located in 2 locus RHD & RHCE • We inherit these genes in groups of three from each parent • A common combination is CDe/cde • Other individuals have combinations of cDE, cde, Cde, cdE
Rh System • D Positive are either D/D or D/d • D Negative are d/d • 85% of the population are D Positive • 15% of the population are D Negative • Other Rh antigens discovered and named C,c,E and e • Weak D phenotype • Rhnull
Weak D Phenotype (Du) The weak D phenotype is thought to occur by one of three mechanisms: (a) inheritance of an RHD gene encoding for a weakened expression of D (DCe or DcE) (b) interaction of the D gene with other genes (Dce/Ce) (c) inheritance of an RHD gene missing some epitopes. (lack of part of D)
Hemolytic Disease of the Newborn (HDN) (Erythroblastosis fetalis)
Background • A French midwife was the first to report hemolytic disease of the newborn (HDN) in 1609. • In 1932, Diamond and colleagues described the relationship of fetal hydrops, jaundice, anemia, and erythroblasts in the circulation, a condition later called erythroblastosis fetalis. • Levine later determined the cause after Landsteiner and Weiner discovered the Rh blood group system in 1940. • In 1953, Chown subsequently confirmed the pathogenesis of Rh alloimmunization to be the result of passage of Rh-positive fetal red blood cells after transplacental hemorrhage into maternal circulation that lacked this antigen.
Rh Incompatibility • Expression is limited to RBCs • Rh positive: 45% are homozygous and 55% are heterozygous • Rh incompatibility is a condition which develops when there is a difference in Rh blood type between that of the pregnant mother (Rh negative) and that of the fetus (Rh positive). • After the initial exposure to a foreign antigen, the maternal immune system produces antibodies of the immunoglobulin M (IgM) isotype that do not cross the placenta, and later it produces antibodies of the IgG isotype that traverse the placental barrier.
ABO incompatibility • ABO incompatibility is limited to type O mothers with fetuses who have type A or B blood • in type O mothers, the antibodies are predominantly IgM in nature • Because A and B antigens are widely expressed in a variety of tissues besides RBCs, only small portion of antibodies crossing the placenta is available to bind to fetal RBCs. In addition, fetal RBCs appear to have less surface expression of A or B antigen, resulting in few reactive sites—hence the low incidence of significant hemolysis in affected neonates.
Causes • Common causes for HDN • Rh system antibodies • ABO system antibodies • Uncommon causes Kell system antibodies • Rare causes • Duffy system antibodies • MNS and s system antibodies • No occurrence in HDN • Lewis system antibodies • P system antibodies
BEFORE BIRTH • Antibodies cause destruction of the red cells • Anemia • heart failure • fetal death
AFTER BIRTH • Antibodies cause destruction of the red cells • Anemia • Heart failure • Erythroblastosis • General edema Called hydrops fetalis and erythroblastosis fetalis • Build up of billirubin • Kernicterus • Severe retardation
Kernicterus due to hyperbilirubinemia due to erythroblastosis fetalis due to Rh incompatibility
بیلی روبین: • (1) interruption of normal neurotransmission (inhibits phosphorylation of enzymes critical in release of neurotransmitters) (2) mitochondrial dysfunction • (3) cellular and intracellular membrane impairment (billirubin acid affects membrane ion channels and precipitates on phospholipid membranes of mitochondria • (4) interference with enzyme activity (binds to specific billirubin receptor sites on enzymes).
PREVENTION • Before birth • Work up mother for risk and evaluation of complications • After birth • Rh immune globulin - IgG anti-D given to prevent primary immunization
Before birth workup • Identify women at risk • ABO - Rh -(Du) - Antibody screen • based on results continue testing (Handout) • IgM antibodies are insignificant • IgG antibodies - titer - freeze and store - retiter with a second sample - looking for a 1:32 rise or change in titer
Before birth workup • titer identifies mothers who need amniocentesis • titer every 4 week until 24th week - then every 2 weeks • amniocentesis is performed after 21st week on high titer - high mortality
Amniocentesis • Analyze pigment that indicates increased hemolysis • Measure OD from 350 - 700 and plot as a function of wavelength • Draw straight line and obtain difference in OD at 450