Download
1 / 24
300 likes | 614 Views
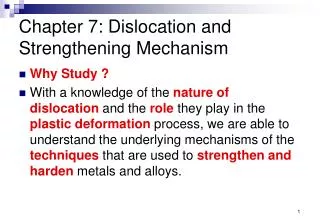
Case Study: Chronic Anterior Shoulder Dislocation. Nicole Boyko, PT/s. Carolyn Michalski, PT/s. Bridget Promaulayko, PT/s. Introducing Joe Shoulder History of Present Condition. 28 y/o English-speaking single white male

E N D
Case Study: Chronic Anterior Shoulder Dislocation Nicole Boyko, PT/s Carolyn Michalski, PT/s Bridget Promaulayko, PT/s
Introducing Joe ShoulderHistory of Present Condition • 28 y/o English-speaking single white male • 2 wks s/p (L) ant shld dislocation incurred while reaching for stationary object from moving vehicle • Manual relocation performed under anesthesia in ER • Pt D/C’d with sling and pain medications • Presents to PT for conservative trial of therapy in hopes of avoiding surgery
History Continued • Long hx of prior (L) ant shld dislocations x 4 • PMH significant for multiple sports-related fx/sprains • FH significant for father with chronic (R) ant shld instability, s/p capsulorraphy • Triathlete, actively training prior to injury • Currently unemployed finance investor • SH noncontributory
PT Tests and Measures • Upper Qtr Screen: (-) for cervical involvement • Motor Control: • Delayed scapular mvmt with GH elevation • Posture: • Prominent ant humeral heads (B) • Mild-mod winging scapulae (L)>(R) • Mild FHP
PT Tests and Measures cont’ • Pain: • Dull ache of (L) shld 4/10, intermittently at rest and after activity • sharp pain with ER, abd, 6/10 • Jt Mobility: (R) (L) • Posterior Glide 2/6 1/6 • Anterior Glide 4/6 5/6 • Superior Glide 2/6 2/6 • Inferior Glide 3/6 4/6
PT Tests and Measures cont’ • Function • Drives short distances • Difficulty with overhead tasks • Sensation • Intact lt touch C2-T1 • Numbness/tingling (L) UE • Special Tests • + apprehension (L) • + ant load & shift, ant drawer & mild impingement • + relocation test • (-) drop arm, empty can
PT Tests and Measures cont’ Muscle Performance/ROM
Relocation Test • Pt in supine • Shld is abducted/ER • Use edge of table as fulcrum • Test (+) for anterior instability if apprehension demonstrated & relieved by posterior stress on shld Mahaffey et al (1999)
Relocation Test • Speer et al (1994) • All subjects had singular dx • Subjects undergoing surgery; able to visually confirm dx • Overall accuracy • <50% pain alone • >80% apprehension alone
Diagnosis • Pattern 4D: Impaired Joint Mobility, Motor Function, Muscle Performance, and Range of Motion Associated with Connection Tissue Dysfunction • ICD-9 Code 831- Shoulder Dislocation
Prognosis • Predicted Optimal Level of Improvement • Training for triathlon with modifications • Home activities/ADLS with min-no pain • Sufficient shld stability to avoid surgery
Prognosis • Predicted Interval Levels of Improvement • Pt will perform 3x10 reps shld ER in scaption with green (intermediate) t-band to fatigue x 4 wks • Pt will perform 3 x 10 reps shld IR in scaption with blue (mod) t-band to fatigue in 4 wks • Pt will show decreased signs of apprehension as seen with performance of D2 PNF pattern with 2 lb pulley weight • PT will be able to flex and abduct (L) shld to 170 with min-no pain allowing for (I) ADLs such as overhead reaching and dressing.
Plan of Care • Frequency/Duration: 2 x/wk x 8 wks • Criteria for Discharge • Return to 90% premorbid function with necessary modifications • 90% ROM of unaffected side • 4+/5 mm strength or greater • Proper mm length-tension relationships • Pain less than or equal to 2/10 • (I) home exercise program
Interventions • Patient-related instruction • Periodic reassessment of HEP- written instructions • Injury prevention and sports modification • Direct Interventions • Therapeutic Exercise • Functional Training • Manual Therapy Techniques • Electrotherapeutic Modalities • Physical Agents and Mechanical Modalities
Phases of Rehabilitation • Phase I: • Rest and immobilization • Pain ctl with NSAIDs • Ice applied to shld • Phase II (begin PT): • Isometrics • Isotonics • Body mechanics/ergonomics • Emphasis on increasing fxnl mvmt • Stability exercises • PNF • Proprioceptive awareness
Phases of Rehabilitation • Phase III: • Endurance • Progressive strengthening • High-level activity challenging shld in open-packed position • Phase IV: • Sports specific activities
Selected Intervention • Scapular stability exercise • Provide dynamic restraint to anterior translation • Key muscles include subscapularis, traps and serratus anterior • Exercises to target • Subscapularis Isometric Exercise • Push ups with a plus Hall and Brody (1999) p. 612
Rationale • Shoulder mobility requires stable base • Normal scapulohumeral rhythm 2:1 ratio • Rehab should emphasize restoring normal physiological patterns • Scapular stability exercises • Early isometrics and scapular setting • CKC exercises to re-establish normal motor firing patterns • 4 core exercises target all 8 scapular muscles: scaption, push-up plus, press-up, rowing Townsend et al (1991) Mosley et al (1992) Kibler (1998) Decker et al (1999)
Selected Interventions • Sports specific exercise • Shoulder PNF • D2 pattern for swimming stroke • Concentric/Eccentric • Theraband • Manual resistance • Pulleys
Rationale • Biomechanics of freestyle swim stroke • Forceful concentric IR/add through acceleration phase • Eccentric activation of ER in follow-through phase • Unique characteristics of swimmers • Excessive external rotation ROM • Limited internal rotation ROM, post capsule or cuff tightness • ER: IR ratio typically lower in swimmers than normal subjects 2° selective strengthening of IR • Higher ER: IR ratio found in overhead athletes with instability
Rationale • Sports-specific rehab should include: • Balanced exercises for the rotator cuff and scapular muscles (serratus ant, traps) • Stretching post structures to prevent further reduction in IR ROM being cautious not to stretch beyond frontal plane to avoid excessive ant displacement • Stroke modifications: increasing body roll, maintaining high elbow, avoiding excessive elbow extension before beginning hand insweep Black et al (1997); McMaster et al (1998); Rupp et al (1995)
Outcome • Joe was able to avoid surgery and return to training • He went on to win the Ironman in Hawaii • Look for Joe in Athens in the 2004 Summer Olympics!