Download
1 / 25
340 likes | 1.48k Views
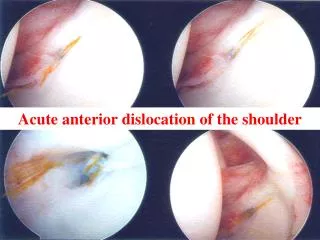
Management of Acute Shoulder Dislocation. An overview Heather Campion Sports Medicine Conference 1/22/08. Incidence. Shoulder is the most commonly dislocated joint Traumatic Dislocations Anterior 96% Posterior 2-4% Diverse group of patients experience dislocations; M and F

E N D
Management of Acute Shoulder Dislocation An overview Heather Campion Sports Medicine Conference 1/22/08
Incidence • Shoulder is the most commonly dislocated joint • Traumatic Dislocations • Anterior 96% • Posterior 2-4% • Diverse group of patients experience dislocations; • M and F • young and old • active and inactive
Anatomic Consideration • Glenohumeral stabilization mechanisms • Passive: joint conformity, vacuum effect, ligamentous and capsular restraints, labrum • Active: long head of Biceps and Rotator Cuff • Pathoanatomy of shoulder dislocations • Bankart Lesion: avulsion of anteroinferior labrum • Hill-Sachs Lesion: posterolateral humeral head defect • Assoc. RCT: more common in older patients
Clinical Evaluation • PE: • Prominent acromion, sulcus sign, palpable humeral head anteriorly • Neuro integrity of axillary and musculcutaneous nerves • Apprehension Test: reproduces sense of instability and pain in shoulder reduced prior to exam
Radiographic Evaluation • AP vs true AP • Axillary vs Valpeau Axillary • Special Views: • West Point axillary: for visualization of glenoid rim • Hill-Sach view: internal rotation view • Stryker Notch: view 90% of posterolateral humeral head
Management • Pre-Medication • Reduction Maneuvers • Post-Reduction Immobilization
Pre-Medication • Methods of Premedication prior to Reduction • None • Intraarticular Lidocaine • IV Sedation • Supraclavicular Block • Suprascapular Block
IV Sedation vs Intraarticular Lidocaine Injection • Level 1 RCT: Miller et al JBJS 2002 • Prospective Randomized study put isolated shoulder dislocation patients (#30) into 2 groups • Variety of Outcome Measures: • Reduction Success • Complications • Pain • Time to reduce/Time in the ER • Cost
IV Sedation vs Intraarticular Lidocaine Injection • No significant difference between: • Reduction Success • Reduction Time • Pain Score • Statistical Significance: • Pts tx with intraarticular Lidocaine • left the ER earlier • Fewer Complications • Lower Cost with Lidocaine
IV Sedation vs Intraarticular Lidocaine Injection Intra-articular Lidocaine Injection is Preferred over IV Sedation
Reduction Maneuvers • Is there an Ideal Method for Reduction? • Over 24 Techniques Described • Most Common Techniques • Kocher (71-100%) • External Rotation (78-90%) • Milch (70-89%) • Stimson (91-96%) • Traction/Countertraction • Scapular Manipulation (79-96%)
Kocher Maneuver • Arm is adducted and flexed at the elbow • Externally rotate arm until resistance is felt • The ER arm is flexed forward as far as possible • The arm is internally rotated
External Rotation • Arm aducted to body • Forearm flexed to 90 degrees • Traction on forearm • Gentle and gradual external rotation until reduction
Milcher Technique • Patient is supine • One hand on shoulder, with thumb on dislocated humeral head • Other arm slowly abducts shoulder to overhead position • Head is gently pushed over glenoid rim to reduce dislocated shoulder
Stimson Technique • Patient is supine • Affected arm hanging down over the edge • 10 lbs weight applied to wrist • Wait for relaxation and auto-reduction
Traction/Countertraction • Arm in some abduction • Traction applied to arm • Assistant applies firm counter-traction with sheet across the body
Scapular Manipulation • Patient is prone • Shoulder flexed to 90 degrees hanging with elbow flexed and humerus in external rotation • 5-15lbs of traction on arm • One hand on superior scapula pushing laterally • Other hand on inferior angle pushing medially
Milch vs Kocher • RCT (Beattie 1986) • Randomization by date • 111 patients • No premedication • Outcome: Successful Reduction • Results: No difference in manuever for successful reduction
Is there a best Reduction Maneuver? • Unknown: More Research Needed • Recommend learning three techniques and gaining experience with them each
Post-Reduction Immobilization • Is immobilization necessary? • What Method is Best?
Does immobilization reduce recurrence? • Level I RCT: Hovelius JBJS 2008 • Prospective multi-center study • 257 primary anterior shoulder dislocations • 25 year follow up • Results: Immobilization for 3-4 weeks after shoulder dislocation does NOT change the prognosis compared with immediate mobilization
Internal vs External Rotation • Level II RCT: Itoi JBJS 2007 • Basis: MRI has shown that coaptation of the Bankart lesion is better with the arm in ER than in IR • Thought: If the Bankart heals recurrence is less likely • 198 primary shoulder dislocations randomized to ER or IR immobilization for 3 weeks • Followed for a minimum of 2 years • Level 2: low compliance, instructional bias, short f/u
Internal vs External Rotation • Level II RCT: Itoi JBJS 2007 • ER for 3 weeks • Recurrence rate: 32% • IR for 3 weeks • Recurrence rate: 60% • P = 0.007
Conclusion • Premedicate with Intraarticular Lidocaine • Learn multiple reduction maneuvers • If you decide to immobilize, immobilize in ER