Download
1 / 1
10 likes | 177 Views
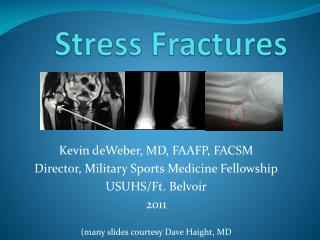
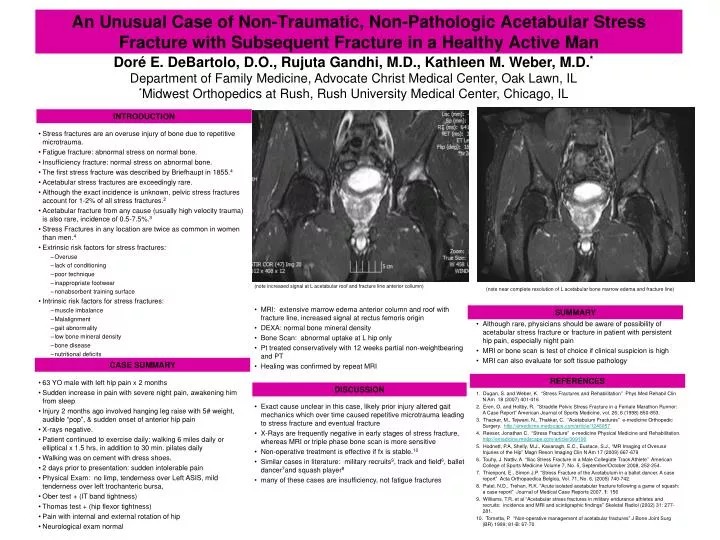
An Unusual Case of Non-Traumatic, Non-Pathologic Acetabular Stress Fracture with Subsequent Fracture in a Healthy Active Man. Doré E. DeBartolo, D.O., Rujuta Gandhi, M.D., Kathleen M. Weber, M.D. * Department of Family Medicine, Advocate Christ Medical Center, Oak Lawn, IL

E N D
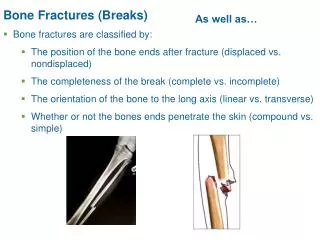
An Unusual Case of Non-Traumatic, Non-Pathologic Acetabular Stress Fracture with Subsequent Fracture in a Healthy Active Man Doré E. DeBartolo, D.O., Rujuta Gandhi, M.D., Kathleen M. Weber, M.D.* Department of Family Medicine, Advocate Christ Medical Center, Oak Lawn, IL *Midwest Orthopedics at Rush, Rush University Medical Center, Chicago, IL INTRODUCTION (note near complete resolution of L acetabular bone marrow edema and fracture line) • Although rare, physicians should be aware of possibility of acetabular stress fracture or fracture in patient with persistent hip pain, especially night pain • MRI or bone scan is test of choice if clinical suspicion is high • MRI can also evaluate for soft tissue pathology 1. Dugan, S. and Weber, K. “Stress Fractures and Rehabilitation” Phys Med Rehabil Clin N Am 18 (2007) 401-416 2. Eren, O. and Holtby, R. “Straddle Pelvic Stress Fracture in a Female Marathon Runner: A Case Report” American Journal of Sports Medicine, vol. 26; 6 (1998) 850-853. 3. Thacker, M., Tejwani, N., Thakkar, C. “Acetabulum Fractures” e-medicine Orthopedic Surgery. http://emedicine.medscape.com/article/1246057 4. Reeser, Jonathan C. “Stress Fracture” e-medicine Physical Medicine and Rehabilitation. http://emedicine.medscape.com/article/309106 5. Hodnett, P.A, Shelly, M.J., Kavanagh, E.C., Eustace, S.J., “MR Imaging of Overuse Injuries of the Hip” Magn Reson Imaging Clin N Am 17 (2009) 667-679 6. Touhy, J. Nattiv, A. “Iliac Stress Fracture in a Male Collegiate Track Athlete” American College of Sports Medicine Volume 7, No. 5, September/October 2008, 252-254. 7. Thienpont, E., Simon J.P. “Stress Fracture of the Acetabulum in a ballet dancer. A case report” Acta Orthopaedica Belgica, Vol. 71, No. 6, (2005) 740-742. 8. Patel, N.D., Trehan, R.K. “Acute isolated acetabular fracture following a game of squash: a case report” Journal of Medical Case Reports 2007, 1: 156 9. Williams, T.R. et al “Acetabular stress fractures in military endurance athletes and recruits: incidence and MRI and scintigraphic findings” Skeletal Radiol (2002) 31: 277-281. 10. Tornetta, P. “Non-operative management of acetabular fractures” J Bone Joint Surg (BR) 1999; 81-B: 67-70 (note increased signal at L acetabular roof and fracture line anterior collumn) • MRI: extensive marrow edema anterior column and roof with fracture line, increased signal at rectus femoris origin • DEXA: normal bone mineral density • Bone Scan: abnormal uptake at L hip only • Pt treated conservatively with 12 weeks partial non-weightbearing and PT • Healing was confirmed by repeat MRI • Exact cause unclear in this case, likely prior injury altered gait mechanics which over time caused repetitive microtrauma leading to stress fracture and eventual fracture • X-Rays are frequently negative in early stages of stress fracture, whereas MRI or triple phase bone scan is more sensitive • Non-operative treatment is effective if fx is stable.10 • Similar cases in literature: military recruits9, track and field6, ballet dancer7and squash player8 • many of these cases are insufficiency, not fatigue fractures • Stress fractures are an overuse injury of bone due to repetitive microtrauma. • Fatigue fracture: abnormal stress on normal bone. • Insufficiency fracture: normal stress on abnormal bone. • The first stress fracture was described by Briefhaupt in 1855.4 • Acetabular stress fractures are exceedingly rare. • Although the exact incidence is unknown, pelvic stress fractures account for 1-2% of all stress fractures.2 • Acetabular fracture from any cause (usually high velocity trauma) is also rare, incidence of 0.5-7.5%.3 • Stress Fractures in any location are twice as common in women than men.4 • Extrinsic risk factors for stress fractures: • Overuse • lack of conditioning • poor technique • inappropriate footwear • nonabsorbent training surface • Intrinsic risk factors for stress fractures: • muscle imbalance • Malalignment • gait abnormality • low bone mineral density • bone disease • nutritional deficits • 63 YO male with left hip pain x 2 months • Sudden increase in pain with severe night pain, awakening him from sleep • Injury 2 months ago involved hanging leg raise with 5# weight, audible “pop”, & sudden onset of anterior hip pain • X-rays negative. • Patient continued to exercise daily: walking 6 miles daily or elliptical x 1.5 hrs, in addition to 30 min. pilates daily • Walking was on cement with dress shoes. • 2 days prior to presentation: sudden intolerable pain • Physical Exam: no limp, tenderness over Left ASIS, mild tenderness over left trochanteric bursa, • Ober test + (IT band tightness) • Thomas test + (hip flexor tightness) • Pain with internal and external rotation of hip • Neurological exam normal SUMMARY CASE SUMMARY REFERENCES DISCUSSION