Download
1 / 98
980 likes | 1.25k Views
Biology 221 Anatomy & Physiology II. TOPIC 7 Respiratory System. Chapter 23 pp. 834-879. E. Lathrop-Davis / E. Gorski / S. Kabrhel. Functions. The main function of the respiratory system is exchange gases, especially O 2 and CO 2 . Other functions of the respiratory system include:

E N D
Biology 221 Anatomy & Physiology II TOPIC 7Respiratory System Chapter 23 pp. 834-879 E. Lathrop-Davis / E. Gorski / S. Kabrhel
Functions • The main function of the respiratory system is exchange gases, especially O2 and CO2. • Other functions of the respiratory system include: • maintaining acid-base (pH) balance (CO2 + H2O H2CO3); • sound production (vocalizations); • neurotransmitter removal; • conversion of angiotensin I to angiotensin II; • housing olfactory receptors for smell; and • trapping and dissolving small clots before they reach the systemic circulation.
Basic Processes of Respiration The four basic processes of respiration are: • ventilation, which moves air into and out of the lungs; • external respiration, which is theexchange of gases between blood and air in lungs; • blood gas transport, which is the transport of gases between lungs and body tissues; and • internal respiration, which is the exchange of gases between blood and body tissues. Fig. 23.17, p. 860
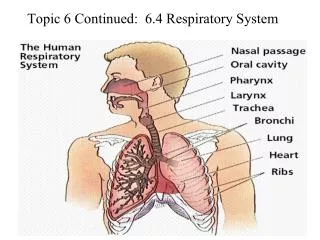
Basic Airway Organization There are two major groups of passageways. • Conducting passageways move air into and out of body but are not involved in actual gas exchange • Conducting passageways include the nose, pharynx, trachea, larynx, bronchi, bronchioles, and terminal bronchioles. • Respiratory passageways are involved in the exchange of gases between air and blood. • Respiratory passageways include the respiratory bronchioles, alveolar ducts, and alveoli. Fig. 23.1, p. 836
Lung Anatomy • The lungs are located in the thoracic cavity lateral to mediastinum. • Each lungs consists of lobes. There are 3 on the right and 2 on left. Lobes are served by secondary bronchi. • Each lobe consists of several bronchopulmonary segments, sections of lobes separated by connective tissue. • Each bronchopulmonary segment is served by its own tertiary (segmental) bronchus. • Each bronchopulmonary segment is supplied by its own artery, vein, and lymphatics. • Each segment can be removed surgically with limited affects on the surrounding segments. See Fig. 23.10, p. 848
Lung Anatomy • Bronchopulmonary segment are divided into lobules, which are the smallest visible subdivisions of lung tissue. Lobules are served by large bronchioles. • Lung tissue consists of air passageways and respiratory surfaces embedded in elastic connective tissue. • The hilus is an indentation on the medial surface of the lung through which bronchi, blood vessels, lymphatics and nerves pass. See Fig. 23.10, p. 848
Lung Anatomy (con’t) • Serous membranes cover the lungs and line the thoracic cavity. • The visceral (= pulmonary) pleura covers lungs. • The parietal pleura lines the thoracic cavity. • The “space” between them is pleural cavity. This space is filled with serous fluid. • Think About It: What is one important function of this fluid? (See A&P I Unit 2 – Tissues) See Fig. 23.10, p. 848
Conducting Passageways: Nose and Nasal Cavity • The functions of the nose and nasal cavity include: • serving as airways for ventilation; • moistening, warming, and filtering air; • resonance of sounds produced for speech; • housing olfactory receptors for smell. Fig. 23.3, p. 838
Conducting Passageways: Nose and Nasal Cavity • Several special structures are associated with the nasal cavity. • The paranasal sinuses aid resonance of sound and lighten the skull. (Covered in lab) • The nasal conchae are covered with mucous membranes and increase the surface area for warming and moistening the air. • The nasal septum separates right and left and helps keep an open passage even when one side is blocked. Fig. 23.3, p. 838
Conducting Passageways: Nose and Nasal Cavity • The palate separates the nasal cavity from the oral cavity. This permits breathing while eating. • The hard palate consists of the palatine process of the maxilla and the palatine bones and is useful during chewing. • The soft palate consists of muscle and closes the opening to the nasopharynx during swallowing. Fig. 23.3, p. 838
Conducting Passageways: Pharynx • The pharynx connects the nose and mouth to the larynx. • The three “parts” of the pharynx are distinguished by landmarks. • The nasopharynx carries air only. • It is located posterior to the nasal cavity, superior to soft palate. • It contains the pharyngeal tonsils (adenoids; see Topic 5). • The auditory tubes (also called the pharyngotympanic or eustachian tubes) open into the nasopharynx. (See A&P I Unit 10) Fig. 23.3, p. 838
Conducting Passageways: Pharynx • The oropharynx is a passage for air and food. • It is posterior to oral cavity, inferior to soft palate. • It is lined with stratified squamous epithelium, which protects against abrasion. • The lingual and palatine tonsils protect against food and air borne particles. (See Topic 5) • The laryngopharynx is a passage for air and food • It is inferior to oropharynx and posterior to the larynx. • It is also lined with stratified squamous epithelium. Fig. 23.3, p. 838
Conducting Passageways: Larynx • The opening into larynx is called the glottis. • The epiglottis is a piece of mucosa-covered elastic cartilage. • It covers the glottis and keeps food out of larynx during swallowing. • The walls of the larynx are formed by pieces of hyaline cartilage including: • the thyroid cartilage, which is the largest, • the cricoid cartilage, and • the arytenoid cartilages, which are important to sound production.
Larynx: Sound Production • The true vocal cords (folds) are folds of mucosa containing elastic vocal ligaments that vibrate to produce sound. • Tension is controlled by arytenoid cartilages • The vocal cords tighten during exhalation and air movement causes vibration of cords. • Pitch (frequency) is controlled by changing length and tension of cords. • Tighter stretch produces higher frequency. • Loudness depends on force of vibration. • Vestibular folds, located superior to the vocal folds, protect the vocal folds.
Conducting Passageways: Trachea • The airways from from the larynx to the level of the T5 vertebra in the chest are patent. That is, they are kept open to allow free flow of air. • The trachea contains 16-20 hyaline cartilage rings. • These rings are incomplete in back, which makes for easier passage of food through the esophagus. Fig. 23.5, p. 843
Conducting Passageways: Trachea There are 3 layers in trachea wall. • The mucosa consists of ciliated pseudostratified columnar epithelium with goblet cells and an underlying lamina propria of areolar connective tissue. • Goblet cells in the epithelium produce mucus that helps trap airborne particles. • Cilia form ciliary escalator, which moves the particle-laden mucus upwards. • The submucosa consists of connective tissue layer. • Seromucous glands secrete additional mucus.
Conducting Passageways: Trachea • The adventitia consists of elastic connective tissue and hyaline cartilage rings. • The rings are incomplete posteriorly. • The trachealis muscle consists of smooth muscle and bridges the rings posteriorly.
Bronchial Tree • The bronchial tree includes both conducting and respiratory passageways. • Conducting passageways include the primary bronchi through the terminal bronchioles. • Respiratory passageways include the respiratory bronchioles, which lead to the alveoli. • General trends include: • a decrease in and eventual loss of cartilage rings; • the gradual addition of smooth muscle to control airway diameter; and • flattening of the epithelium, which goes from pseudostratified columnar to simple squamous.
Conducting Passageways: Primary Bronchi • One primary bronchus goes to each lung. • The walls have cartilage with some smooth muscle. • The bronchi are lined with pseudostratified ciliated columnar epithelium with numerous goblet cells. Fig. 23.7, p. 844
Conducting Passageways: Secondary Bronchi • Secondary bronchi are branches of the primary bronchi. These serve the lobes of lungs; there are 3 on right and 2 on left. (See pg. 5) • Walls have less cartilage and more smooth muscle than do the primary bronchi. • The secondary bronchi are lined with pseudostratified ciliated epithelium in which cell height is smaller than in the primary bronchi. http://www.pul.unimaas.nl//respir.htm#lower%20tract Fig. 23.7, p. 844
Conducting Passageways: Tertiary Bronchi • Tertiary bronchi are branches of the secondary bronchi and serve the bronchopulmonary segments. • The walls have irregular rings of cartilage and much more smooth muscle. • Cells of the pseudostratified ciliated epithelium lining are very short. Fig. 23.7, p. 844 http://www.pul.unimaas.nl//respir.htm#lower%20tract
Conducting Passageways: Bronchioles • Bronchioles are small branches of the tertiary bronchi. • There are many subdivisions and levels of bronchioles. • The walls consist mainly of smooth muscle with little or no cartilage. This muscle will be important to control of airway diameter. • Bronchioles are lined with cuboidal epithelium. Fig. 23.7, p. 844 http://www.pul.unimaas.nl//respir.htm#lower%20tract
Conducting Passageways: Terminal Bronchioles • Terminal bronchioles are branches deep in the lungs. • They lack cartilage and smooth muscle is scattered. • Terminal bronchioles are lined with cuboidal epithelium. • Terminal bronchioles are the last of the conducting passageways and lead to respiratory bronchioles. Fig. 23.7, p. 844 http://www.pul.unimaas.nl//respir.htm#lower%20tract
Respiratory Zone (Passageways) Respiratory Bronchioles • Respiratory bronchioles are the smallest and thinnest of air passageways leading to respiratory surfaces of lung. • They are lined with low simple cuboidal epithelium. Fig. 23.8, p. 845 http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm
Respiratory Zone: Alveoli • Alveolar ducts are passageways from the respiratory bronchioles to the alveolar sacs and alveoli. • Alveolar sacs are groups of alveoli with a common opening. • Alveoli (singular = alveolus) are the individual air sacs. http://www.usc.edu/hsc/dental/ghisto/lng/d_28.html Fig. 23.8, p. 845
Respiratory Zone: Alveoli • Thin-walled structures across which gases are exchanged • Barrier to diffusion respiratory gases (CO2 and O2) • Adjacent alveoli joined by alveolar pores http://www.usc.edu/hsc/dental/ghisto/lng/d_28.html Fig. 23.8, p. 845
Respiratory Zone: “Respiratory Membrane” • The respiratory membrane is the surface across which gases are exchanged. • It consists of the alveolar epithelium, the capillary epithelium, and the basement membrane between them. • Alveolar endothelium consists of two types of cells. • Type I cells are simple squamous epithelium (blue arrow in the linked image) and function in gas exchange. • Type II cells are scattered simple cuboidal cells (green arrow in the linked image) and secrete surfactants. http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm (#15)
Respiratory Zone: “Respiratory Membrane” • The basal lamina is the basement membrane that joins the two epithelial layers. • Capillary endothelium consists of simple squamous epithelium. http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm
Nerve Supply to Lungs • Nerves enter and leave through the hilus. • Pulmonary plexuses provide autonomic (ANS) innervation to smooth muscle of the bronchi and bronchioles. There are two kinds of plexuses – one for each division of the ANS. • The sympathetic pulmonary plexus provides sympathetic innervation that leads to dilation of bronchi and bronchioles. • Think About It: Why would this be important to the fight or flight response? Fig. 14.4, p. 519
Nerve Supply to Lungs • Parasympathetic innervation from the pulmonary plexus of the Vagus (X) nervecauses constriction of bronchi and bronchioles. • Think About It: Which division (sympathetic or parasympathetic) would be involved in responses to airborne irritants? • (HINT: The response to irritants is to decrease the size of the airways.) Fig. 14.4, p. 517
Blood Supply to Lungs • Vessels enter and leave through the hilus. • Two systems serve the lungs. • The pulmonary circulation carries blood to the respiratory surfaces of the lungs for gas exchange with air in alveoli. • Pulmonary arteries bring blood to the lungs. • Alveolar capillaries are sites of exchange of gases between air in the alveoli and blood. • Pulmonary veins carry blood from the lungs to the heart. • Recall: Which of these vessels carry oxygenated blood? Which ventricle pumps into this system? Which atrium receives blood from it?
Blood Supply to Lungs • The bronchial circulation carries blood to all lung tissues except the alveoli. • This circulation goes from the aorta to bronchial arteries to capillaries to bronchial veins. • Most blood returns via pulmonary veins due to numerous anastomoses. • Recall: Which of these vessels carry oxygenated blood? Which ventricle pumps into this system? Which atrium receives blood from it?
Ventilation • Ventilation is the movement of air into or out of lungs. • Inspiration is movement of air into the lungs. • Expiration is movement of air into the lungs. • Air flow is directly related to the pressure gradient; and inversely related to resistance. • Air moves from areas of higher pressure to areas of lower pressure. • The pressure gradient moves air and gases between nose (or mouth) and the terminal bronchioles. • Between the terminal bronchioles and alveoli, individual gas movement is driven by diffusion.
Ventilation: Pressures 3 pressures are involved in ventilation. • Atmospheric pressure (PA) is the same as air pressure. • It is the external pressure of the air around the body. • Intrapleural (intrathoracic) pressure is the pressure within the pleural cavity. • Intrapleural pressure is always less than intrapulmonary pressure (within alveoli) by about 4 mm Hg. • If intrapleural pressure equals or exceeds atmospheric pressure, the lungs collapse. • Intrapulmonary (intra-alveolar) pressure (PL) is the pressure within the alveoli.
Ventilation: Pressures • Atmospheric pressure normally stays roughly the same at any given altitude. • Since atmospheric pressure doesn’t change, ventilation (breathing) involves changing intrapulmonary pressure.
Boyle’s Law • Boyle’s law states that gas pressure is inversely proportional to volume (V). • Increasing volume decreases the pressure on the gas. • Decreasing volume increases the pressure on the gas. • Air moves from higher pressure to lower pressure.
Boyle’s Law • Given the pressures: • PL = intrapulmonary pressure • PA = atmospheric pressure • And that air moves from higher to lower pressure. • For inspiration: PL < PA • That is, pressure in the lungs must be less than atmospheric pressure for air to move into the lungs. • Volume, V, must increase so that PL can decrease. • For expiration: PL > PA • That is, pressure in the lungs must be more than atmospheric pressure for air to move out of the lungs. • V must decrease so that PL can increase
Processes of Ventilation • The process of ventilation involves contraction of skeletal muscle. (Review notes from A&P I muscle lab.) • This allows voluntary control as well as subconscious control. • Muscles whose contraction increases the size of the thoracic cavity will cause inspiration. • Relaxation of these muscles will cause passive expiration as they return to their resting state. • Muscles whose contraction decreases the size of the thoracic cavity will add to expiration.
Inspiration • The diaphragm and/or external intercostal muscles contract (innervated by phrenic and intercostal nerves, respectively). • Thoracic volume increases. • Intrapleural pressure decreases. • Lungs expand into the lower pressure thoracic (pleural) cavity. • Intrapulmonary pressure decreases. • Air moves in. Processes of Ventilation
Expiration • The diaphragm and external intercostal muscles relax (passive process) and lungs recoil. • Thoracic volume decreases. • Intrapleural pressure increases. • Lungs are compressed by the increased pressure in thoracic (pleural cavity). • Intrapulmonary pressure increases. • Air moves out. – Expiration is normally passive Processes of Ventilation
“Forced” Air Movements: Expiration • Forced expiration expels more than the normal amount of air. • Forced expiration is accomplished by increasing intrapleural pressure beyond normal breathing by making thoracic cavity even smaller. • The muscles that contribute to forced expiration are: • abdominal muscles – external and internal obliques, transversus abdominis; and • thoracic muscles – internal intercostals, latissimus dorsi, quadratus lumborum.
“Forced” Air Movements: Inspiration • Forced inspiration involves inhaling more than normal amount of air. • This is accomplished by decreasing intrapleural pressure beyond normal breathing by increasing the thoracic cavity even more. • Muscles involved are the: • pectoralis minor, scalenes, sternocleidomastoid muscles.
Promoting Lung Expansion • Inspiration (when inspiratory muscles contract) is aided by two things: compliance and surface tension within the pleural cavity. • Compliance is the ability of the lungs to expand. • Decreased compliance makes it more difficult to inflate the lungs. • Causes of reduced compliance include: • loss of elasticity of lung tissue; and • increased alveolar surface tension.
Promoting Lung Expansion • Surface tension within the pleural cavity is caused by pleural fluid. • Pleural fluid (serous fluid within the pleural cavity) creates negative intrapleural pressure between the pleural membranes (not unlike water between two pieces of glass). • Excess fluid is normally removed by the lymphatic system. • Failure to remove fluid results in a build up of fluid (pulmonary edema), which increases the intrapleural pressure (i.e., it becomes less negative) making it difficult to inflate the lungs.
Promoting Lung Compression • Expiration when inspiratory muscles are relaxing is aided by alveolar fluid surface tension and elastic recoil of the lungs. • Alveolar fluid surface tension causes the lungs to “want” to collapse by pulling the sides of the alveoli closer together. • Surfactant decreases alveolar surface tension, thus preventing collapse. • Respiratory distress syndrome (RDS; also known as hyaline membrane disease of the newborn) occurs in a premature babies that have insufficient amounts of surfactant in lung; the lungs collapse during expiration and must be reinflated.
Promoting Lung Compression • Elasticity is the elastic recoil of lungs due to elastic tissue in the walls of the lungs. • Elasticity helps the lungs become smaller like the deflating of a stretched balloon. • Emphysema is a disease that decreases elasticity. This makes exhalation difficult and instead of being passive, it becomes an active process.
Resistance to Airflow • Resistance to airflow opposes movement of flow into/out of lungs. • Resistance is related to size (radius [r] and length) of the air passageways and viscosity of the “fluid” (air). • Resistance (length of tube x viscosity of fluid) / r4 • Resistance is: • directly related to tube length; • directly related to viscosity; and • indirectly related to radius4 (i.e., 1/r4). • Resistance is greatest in medium-sized bronchioles. Fig. 23.5, p. 854 Means “is approximately equal to”
Factors Increasing Airflow Resistance Increased airflow resistance decreases flow. Things that increase resistance include: • Bronchoconstriction, whichmakes airways narrower • Bronchoconstriction is caused by: • the parasympathetic response to inhaled irritants; • acetylcholine administration; and • decreased PCO2(partial pressure of CO2). • Other factors that decrease size of airways include: • solid obstructing tumors; • mucus accumulation; and • inflammation.
Factors Decreasing Airflow Resistance Decreased airflow resistance increases flow. • Bronchodilation makes airways larger. Bronchodilation is caused by: • sympathetic innervation; • epinephrine administration; and • increased PCO2.
Regulation of Ventilation • Ventilation is controlled by the respiratory center located in the medulla oblongata (as part of the reticular formation). • The respiratory center consists of: • inspiratory center (dorsal respiratory group or DRG); and the • expiratory center (ventral respiratory group or VRG). • Under quiet breathing at rest, breathing is controlled primarily by the DRG.