Download
1 / 37
520 likes | 1.15k Views
AMYLOIDOSIS . When good proteins go bad. HPI . A 69 yo male complains: “I move so slowly that I can’t play golf anymore” . What questions would you like to ask your patient? . HPI. Pt complains of feeling weak and tired for about a year.

E N D
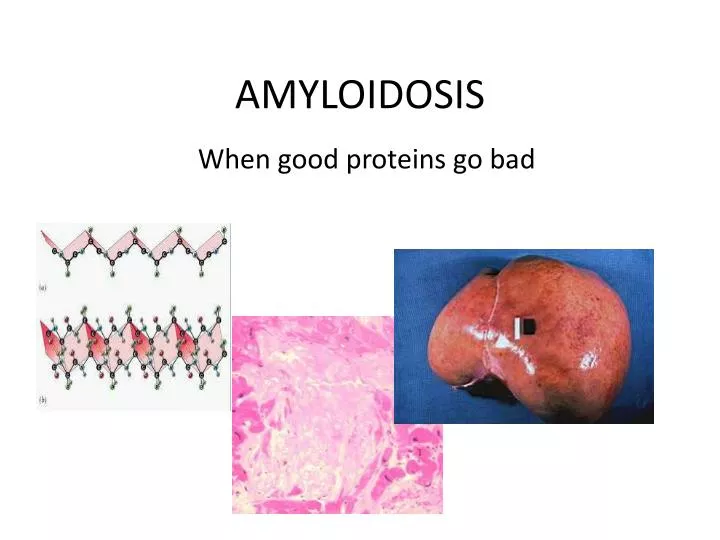
AMYLOIDOSIS When good proteins go bad
HPI A 69 yo male complains: “I move so slowly that I can’t play golf anymore”. What questions would you like to ask your patient?
HPI • Pt complains of feeling weak and tired for about a year. • Pt unintentionally lost 20 pounds in the past 6 months. • Pt complains of one year of worsening dyspnea on exertion. • Pt complains of intermittent two-pillow orthopnea. • Pt admits that his legs have swelled up on occasion over the past year. • Pt complains that his muscles have felt weak for the past year or so. • Pt complains of subjective fatigue and decreased mental acuity. • Pt complains of a mild sense of abdominal fullness for the past year or so. • Pt complains of pain over his hips, and pain over his right ribs; this came on slowly about three months ago.
Medical History • Significant for hypertension, well-controlled with a thiazide diuretic. • Family history: • Father was diabetic, and died of CHF at age 57. • Mother was hypothyroid, and died of breast cancer at 66. • Social History: • Worked as a salesman for a tractor dealership. 20 pack-year smoking history, but quit five years ago. Drinks socially. No illicit drugs.
Physical Exam (significant findings) • Vitals: • T 37ºC, HR 104, RR 16, BP 138/89 • Neurologic: • Dysarthria – pt says this began insidiously in the last 18 months; denies history of stroke. • Dysphagia – same time frame. • HEENT: • Macroglossia • Mucosal pallor • Chest: • crackles over bilateral lung bases • S4 heart sound • Abdomen • Scaphoid abdomen • Liver edge is palpable 6 centimeters below the costal margin • Extremity • 2+ bilateral pitting edema • 4+ strength
Differential Diagnosis of Anemia • This patient is tachycardic and pale. By physical diagnosis, we can guess that heis likely anemic. • Differential Diagnosis: Can be broad. • Iron deficiency anemia (chronic bleeding?) • Nutritional deficiency (vitamin B12, folate) • Malignancy • Blood dyscrasia • Autoimmunity • Hypersplenism • Infection • Red blood cell structural/metabolic defect
Initial Tests/Procedures • Chem 10 (Na+, K+, HCO3-, Cl-, BUN, Cr, Glucose, Ca++, Phosphate, Mg++) • CBC with differential • B-type Natriuretic Peptide – evaluates for heart failure • Liver Enzymes – detects liver damage • X-rays of painful sites – investigate possibility of malignancy
Tests/Procedures 1: Results • Metabolic: • Na+ 140 mEq/L • K+ 5.2 mEq/L • HCO3 16 mEq/L • Cl- 88 mEq/L • BUN 48 mg/dL • Creatinine 3.0 mg/dL • Glucose 100 mg/dL • Ca++ 12.7 mg/dL • Mg++ 2.0 mg/dL • PO4 3.5 mg/dL • CBC: • Hemoglobin: 7.0mg/dL, reticulocytes 0.02% • Hematocrit: 21% • WBC: 8,000/µL – 74% neutrophil, 20% lymph, 4% monocyte, 1% eosinophils, 1% basophils • Platelet: 200,000/µL • BNP • 650 pg/mL • Liver: • AST 105U/L, ALT, 150U/L, AlkPhos 200U/L • WHICH OF THESE VALUES ARE ABNORMAL?
WHICH OF THESE VALUES ARE ABNORMAL? • Metabolic: (Abnormals are in red) • Na+ 140 mEq/L (Normal ≈ 137-145 mEq/L) • K+ 5.2 mEq/L (Normal ≈ 3.5-5.0 mEq/L) • HCO3 16 mEq/L(Normal ≈ 22-26 mEq/L) • Cl- 88 mEq/L (Normal≈ 98-110 mEq/L) • BUN 48 mg/dL(Normal ≈ 7-21 mg/dL) • Creatinine 3.0 mg/dL(Normal ≈ 0.5-1.4 mg/dL) • Glucose 100 mg/dL(Normal ≈ 65-110 mg/dL) • Ca++ 12.7 mg/dL(Normal ≈ 8.9-10.4 mg/dL) • Mg++ 2.0 mEq/L (Normal ≈ 1.5-2.5 mEq/L) • PO4 3.5 mg/dL(Normal ≈ 2.4-4.1 mg/dL)
WHICH ARE ABNORMAL? • CBC: • Hemoglobin: 7.0 mg/dL(Normal male ≈ 13.2-16.2 mg/dL) • Reticulocytes 0.02% (Normal adult ≈ 0.5%-1.5% • Hematocrit: 21% (Normal male ≈ 40-52%) • WBC: 8,000/µL – 70% neutrophil, 24% lymph, 4% monocyte, 1% eosinophils, 1% basophil. (Normal WBC ≈ 4,100-10,900/µL) • Platelet: 200,000 (Normal 140,000-450,000/µL) • BNP • 650pg/dL (Normal <100 pg/dL; 650 pg/dL suggests moderate heart failure). • Liver: • AST 105, ALT, 150, AlkPhos 200. • AST Normal ≈ 5-35 U/L • ALT Normal ≈ 7-56 U/L • AlkPhos Normal ≈ 38-126 U/L
LAB RESULTS, RECAP • Patient has… • Hypercalcemia • Renal Failure • Elevated BUN and creatinine; patient’s hyperkalemia and anion gap metabolic acidosis are consistent. • The BUN/Creatinine ratio is < 20, which suggests intrinsic renal failure. • Anemia • Elevated Liver Enzymes • Congestive Heart Failure • Based on his labs, which category is first in your differential?
Imaging – Patient’s Chest X-Ray First, look at the patient’s clavicle. See how the cortex is highly radiopaque (white), and thick. Next, look at the patient’s fourth rib in the inset. Notice that the superior surface of the rib looks scalloped, and that the opacity of normal cortical bone is not present. This is consistent with a lytic lesion, or a pathologic process causing localized bone loss. This patient likely has a malignancy.
Imaging – Patient’s Abdominal X-Ray Over here, notice that the bone texture is not as uniform. Rather, there are sudden changes from dark to light. These are consistent with the characteristic “punched-out” lytic lesions of multiple myeloma. First, appreciate the relatively uniform “texture” of the bone in this part of the pelvis. No sudden changes in color.
Imaging – Patient’s Skull Film This is a classic view of multiple myeloma. Note the punched-out lytic lesions (arrow and others). The pathophysiology of these lesions involves nests of tumor cells in the bone. Eventually, these lytic lesions may result in pathologic fractures.
Lead Differential Diagnosis • Given the constellation of abnormalities (calcium, renal, anemia, bone disease), you should suspect multiple myeloma. • Diagnostic criteria for multiple myeloma are: • Characteristic clinical and lab abnormalities (CRAB) • Bone marrow biopsy; generally has to show 10% or more plasma cells • Monoclonal (M) protein in serum • Multiple myeloma alone, however, can’t account for his other problems, including heart failure, his hepatomegaly with elevated liver enzymes, his macroglossia, dysphagia, or dysarthria. • Is there a possible link between his likely myeloma and his other problems? The timing of all these problems is suspicious! • What other diagnostic tests would you order?
More tests? • Confirm Myeloma • Serum Protein Electrophoresis • Bone Marrow Biopsy • Further Investigation • Liver biopsy • Renal biopsy • Echocardiogram • Heart biopsy, if echocardiogram suggests certain cardiomyopathies. • Electrocardiogram
Intro to Serum Protein Electrophoresis • 5 peaks typically observed; each corresponds to a group of plasma proteins. • Albumin: most common protein in human serum • Alpha-1: 90% alpha-1 antitrypsin; also thyroid-binding globulin and transcortin • Alpha-2: alpha-2 macroglobulin, ceruloplasmin and haptoglobin • Beta: • Beta-1: transferrins • Beta-2: beta-lipoprotein • Gamma: immunoglobulins and C-reactive protein Albumin Alpha Beta Gamma
Serum Protein Electrophoresis – Our Patient NORMAL • Serum Protein Electrophoresis PATIENT – note the gamma spike. The gamma spike corresponds to an excess of immunoglobulin in this patient’s serum, made by the myeloma cells. Further analysis showed that this immunoglobulin was monoclonal.
Confirming Myeloma: Bone Marrow Biopsy The pathology report returns, stating that the patient’s bone marrow contains 21% plasma cells, establishing a diagnosis of multiple myeloma. You can tell these are plasma cells by… Clock-face chromatin, arranged densely around the periphery of the nucleus. “Perinuclearhof”, or area of clear cytoplasm near the nucleus.
Next Steps… Now to look at the liver, kidney, and heart findings…is there a link between his cardiac findings and his myeloma?
BIOPSY RESULTS Liver biopsy. “Fluffy” pink amyloid; this consists of beta-pleated protein sheets. Remaining hepatocytes
BIOPSY RESULTS Myocytes Heart biopsy Amyloid
BIOPSY RESULTS Renal Biopsy Glomerulus with mesangial deposits of amyloid. A unique property of amyloid is that it stains well with Congo Red dye. Remember: No Congo red staining, no amyloid!!
To confirm… Renal biopsy, stained with Congo Red. Under polarized light, the stain displays apple-green birefringence.
Biopsy Discussion The biopsy establishes the link between the patient’s myeloma and his other problems. The patient is experiencing amyloidosis, which is an uncommon, but devastating systemic manifestation of this malignancy, in which abnormal protein, or “amyloid” aggregates form in numerous organs. The amyloid in this case likely consists of monoclonal light chains made by the malignant plasma cells.
Results Discussion • CARDIAC TESTING: • Patient’s echocardiogram demonstrates severe diastolic dysfunction. • This result is consistent with the tissue diagnosis of amyloidosis, and with his clinical picture of heart failure. • Pathophysiology Note: Amyloidosis stiffens the ventricles, impairing their ability to fill properly during diastole.
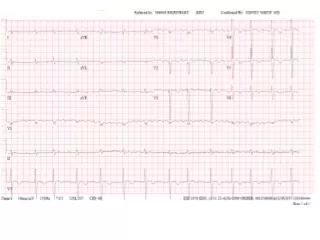
Tests and Procedures: Results • 2 months later patient yields the following EKG. You can tell it’s a complete heart block because the P waves are not paired with QRS complexes. Amyloidosis patients are susceptible to conduction abnormalities due to heart tissue disruption by amyloid. The treatment for complete heart block is a permanent pacemaker.
Our Patient and his Diagnosis • Multiple Myeloma with 2º AL amyloidosis. • Malignancy of Plasma Cells • MM is associated with AL amyloidosis in 20% of biopsy-proven cases. • Most commonly, AL amyloidosis happens as a primary disease, or secondary to other plasma cell dyscrasia syndromes such as MGUS or Waldenströmmacroglobulinemia. • The amyloid consists of fibril-forming or nonfibrillar aggregates of monoclonal immunoglobulin light chains made by the malignant cells.
Amyloidosis • Defined as extracellular deposition of protein fibrils forming beta-pleated sheets. Culprit proteins often originate from plasma. • There are multiple types of amyloidosis, but all amyloid stains with Congo Red dye, which displays apple-green birefringence under polarized light. • Congo Red staining distinguishes amyloidosis from other protein deposition diseases, in which the pathogenic proteins don’t form fibrils.
Amyloidosis • Grossly, involved organs may be enlarged and have a “waxy” or “lardaceous” appearance when cut. Organs may seem unusually firm or heavy. See the small waxy deposits in this cut kidney. Note the distended appearance of this liver.
Amyloidosis See how glossy (waxy) this cut liver looks. Same liver. Arrows point to small pale deposits of waxy material. Early pathologists referred to such organs as “lardaceous”, because they looked as if they were perfused with thick grease.
Amyloidosis • Histologically, amyloid looks amorphous (“fluffy”) on H&E staining, but displays apple-green birefringence when stained with Congo Red.
Amyloidosis • Many different types of amyloidosis have been characterized. • They may occur by themselves (primary amyloidosis) • They may happen in conjunction with another disease (secondary amyloidosis).
Clinical • Amyloid may deposit in any one of a number of organs, with differing results. • Liver: hepatomegaly, elevated enzymes, loss of hepatic function • Kidneys: enlarged kidneys, declining renal function, sometimes proteinuria. • Heart: Restrictive cardiomyopathy • Brain: Amyloidangiopathy • Peripheral Nerves: Neuropathy (muscle weakness, sensory loss) • Skin: Thickening of skin • Tongue: Macroglossia, dysphagia, dysarthria. • Bones/Joints: Arthralgia, arthritis, pathologic fractures.
Treatment • End-organ damage from amyloid is considered to be irreversible (although patients may show some functional improvement during their treatment). • In the case of AL amyloidosis with or without multiple myeloma, the mainstay of treatment is chemotherapy with or without a bone marrow transplant. • If the primary disease process can be halted, then organ transplantation may be an option. • Otherwise, treatment is supportive. • Dialysis and erythropoietin replacement for severe renal failure. • Medications for congestive heart failure may include beta blockers, diuretics, and angiotensin inhibitors. • Pacemaker may be needed if conduction system problems result.
End of Story • The patient is treated medically for his congestive heart failure. • The patient receives a pacemaker for his heart block. • The patient goes on dialysis for his renal failure. • Due to his malignancy, he is not an organ transplant candidate. • The patient is referred to a multiple myeloma specialist for treatment, and is placed on a complex chemotherapy regimen. • Unfortunately, the patient’s prognosis is not good. Average survival for AL amyloidosis plus multiple myeloma is 14 months. By contrast, mean survival with primary AL amyloidosis is 32 months.