Download
1 / 83
930 likes | 1.38k Views
N. S. N. C. Module 2 Hyperacute Stroke Management. Best Practice Nursing Care Across the Acute Stroke Continuum. 1. Hyperacute Stroke Management. This session includes presentations and activities to enhance your learning

E N D
N S N C Module 2Hyperacute Stroke Management Best Practice Nursing Care Across the Acute Stroke Continuum 1
Hyperacute Stroke Management This session includes presentations and activities to enhance your learning The focus is on working with colleagues to discover best ways of using the tools in your clinical settings So, sit back (or stand up) and have fun!!! Welcome! 6/7/2014 2
Hyperacute Stroke Management So, what do you want to get out of this module? Expectations? 6/7/2014 3
Hyperacute Stroke Management Discuss the impact of hyperacute stroke management on patient outcomes Identify your role in pre-hospital and ER stroke care Review the Best Practice Recommendations related to hyperacute stroke management Identify how you can help to implement these at your institution Identify your role in patient and caregiver education Create a stroke care action plan for hyperacute stroke management Objectives 6/7/2014 4
Hyperacute Stroke Management Introduction 15 min Stroke 101(optional) 15 min Pre-Hospital Stroke Care 45 min In the Emergency Room 30 min Break 15 min Hyperacute Stroke Management BPRs 45 min Patient and Family Education 15 min Putting It All Together 30 min Agenda 6/7/2014 5
Hyperacute Stroke Management Continuum of Stroke Care Prevention of strokePublic awareness & patient education Hyperacute stroke management Acute inpatient stroke care Stroke rehabilitation & community reintegration
Hyperacute Stroke Management Continuum of Stroke Care Prevention of strokePublic awareness & patient education Early assessment for stroke rehabilitation should start here Hyperacute stroke management Acute inpatient stroke care Stroke rehabilitation & community reintegration
Hyperacute Stroke Management Acute stroke is a medical emergency and optimizing out-of-hospital care improves patient outcomes EMS plays a critical role in assessment and management Acute interventions such as thrombolysis are time sensitive Why Is This Important? Redirecting ambulances to stroke centres facilitates earlier assessment, diagnosis and treatment which may result in better outcomes. 6/7/2014 8
Canadian Best Practice Recommendations for Stroke Care 2008 • Synthesis of best practice recommendations for stroke care across the continuum • Address critical topic areas • Commitment to keep current and update every two years • First edition released in 2006 • Current update released in 2008 • With four new recommendations • Elaboration of existing ones • www.cmaj.ca December 2, 2008
Stroke 101 Hyperacute Stroke Management Intended only for audiences with no previous knowledge of stroke. 6/7/2014 10
Hyperacute Stroke Management Pre-Hospital Stroke Care 45 min 6/7/2014 11
Hyperacute Stroke Management Your Role in Pre-Hospital Stroke Care At your tables, discuss best practices for effective Pre-Hospital Stroke Care: What information will you need EMS to gather about the patient? What you can do to help rapid assessment & triage in hospital? When done, we'll debrief the whole group to arrive at some best practices Pre-Hospital Stroke Care TABLE ACTIVITY 6/7/2014 12
Hyperacute Stroke Management Patient should be transported without delay to the closest institution that provides emergency stroke care (BPR 3.1) Patient or other members of public must make immediate contact with EMS EMS dispatchers must triage as priority Paramedics should use standardized screening tool Direct transport protocols should be in place Critical information/history should be obtained Receiving facility must be notified EMS Role in Hyperacute Stroke DEBRIEF 6/7/2014 13
Hyperacute Stroke Management From Recognition to Pre-Admission Pre-Hospital Stroke Care Dispatch Detection Delivery Door 14 6/7/2014
Hyperacute Stroke Management Why is the time of onset of the stroke a critical piece of information? Stroke patients who arrive to ER within three and one half hours of symptom onset may be candidates for thrombolytic therapy Hospital destination decisions may be based on time of onset of stroke symptoms Care of Patient with Stroke 15 6/7/2014
Hyperacute Stroke Management A 53-year-old man with a history of hypertension was brought to the ED by paramedics after his employer noticed that he had difficulty with speech, ambulation, and vision. The employer reported that the patient usually left his house at 3:40 am and arrived at work by 4:00 am; however, no one saw him arrive at work and no time clock is used. Paramedics were called at about 5:00 am. What was the time of onset of the stroke? When he went to bed? 3:40 am? 4:00 am? 5:00 am? Last Seen Normal-1 16 CASE STUDY 6/7/2014
Hyperacute Stroke Management What do we know: Patient successfully drove to work; it is unlikely that the stroke began before he left the house. Possible: Symptoms MAY have been very mild at first, that he ignored them, and went to work anyway. Decision: Since we have no evidence for this yet, we TENTATIVELY assign an onset time of 3:40 am, subject to further history. Needed: Find someone at work who saw him and could testify that he was normal or obviously abnormal before the paramedics were called. Last Seen Normal-2 17 CASE STUDY 6/7/2014
Hyperacute Stroke Management Quick identification and screening by pre-hospital providers in the field Blood glucose measurement to exclude hypoglycaemia as a cause of neurological deficit Notification of receiving hospital Transport Treatment to stabilize the patient Pre-Hospital Important Steps 18 6/7/2014
Hyperacute Stroke Management Consistently identifies patients with stroke Evaluate three major findings: Facial droop Arm weakness Speech abnormalities Based on the Cincinnati Stroke Scale or Los Angeles Stroke Scale Key Components of Paramedic Prompt Cards 19 6/7/2014
Hyperacute Stroke Management Patients with 1 of these 3 findings 72% probability of an acute stroke if the symptoms are new Patients with all 3 findings.. 85% probability of an acute stroke if the symptoms are new If the patient has a positive CPSS or one or more of the findings, immediately activate local acute stroke protocol Cincinnati Pre-Hospital Stroke Scale 20 REVIEW 6/7/2014
Hyperacute Stroke Management Pre-Hospital Stroke Care • Symptom Onset • Time • Trauma (history) • Seizure • Neurological Exam • LOC • Pre-Hospital Stroke Scale • Basic Data • Age and gender • Chief complaint • Other tPA exclusions • As per tPA protocol inclusion/exclusion criteria Information obtained and relayed by EMS provider is vital 21 6/7/2014
Hyperacute Stroke Management NIH Stroke Scale 6/7/2014 22 Standard assessment tool for measuring neurologic deficit Measures level of consciousness, best gaze, visual, facial palsy, motor function, language, dysarthria, extinction and inattention Can be used to quantify neurologic function in specified categories at various time points
Hyperacute Stroke Management NIH Stroke Scale EXAMPLE 6/7/2014 23 Source: www.ninds.nih.gov
Hyperacute Stroke Management NIH Stroke Scale EXAMPLE 6/7/2014 24 Source: www.ninds.nih.gov
Hyperacute Stroke Management Canadian Neurological Scale was designed as a simple clinical tool to evaluate the neurological status of acute-stroke patients Measures level of consciousness, orientation, speech and motor functions CNS Stroke Scale 6/7/2014 25
Hyperacute Stroke Management CNS Stroke Scale EXAMPLE 6/7/2014 26
Hyperacute Stroke Management Check Up Quiz EXAMPLE
Hyperacute Stroke Management Check Up To the nearest institution that provides emergency stroke care In hyperacute stroke management, EMS should transport a patient without delay to what type of institution? 6/7/2014 28
Hyperacute Stroke Management Check Up Detection, Dispatch, Delivery, Door What are the four steps in pre-hospital stroke care from recognition to pre-admission? 6/7/2014 29
Hyperacute Stroke Management Check Up Detection, Dispatch, Delivery, Door What are the four steps in pre-hospital stroke care from recognition to pre-admission? 6/7/2014 30
Hyperacute Stroke Management Check Up Stroke patients who can be diagnosed with a CT within three hours of symptom onset may be candidates for thrombolytic therapy Why is the time of onset of the stroke a critical piece of information? 6/7/2014 31
Hyperacute Stroke Management Check Up To exclude hypoglycaemia as a cause of neurological deficit Why is blood glucose measurement so important? 6/7/2014 32
Hyperacute Stroke Management Check Up • Facial droop • Arm weakness • Speech abnormalities What does the Pre-Hospital Stroke Scale measure? 6/7/2014 33
Hyperacute Stroke Management Check Up • 85% probability What is the probability of acute stroke if a patient is abnormal on all three of the Cincinnati measures and symptoms are new? 6/7/2014 34
Hyperacute Stroke Management Check Up Level of consciousness, best gaze, visual, facial palsy, motor function, language, dysarthria, extinction and inattention What does the NIH Stroke Scale measure? 6/7/2014 35
Hyperacute Stroke Management Check Up Level of consciousness, orientation, speech and motor functions What does the Canadian Neurological Scale measure? 6/7/2014 36
In the Emergency Room 30 min
Hyperacute Stroke Management 7-Step Stroke “Chain of Survival” Delivery Dispatch Detection Door Intervention Data Decision
Hyperacute Stroke Management Treatment in the ER is only the start Patients will have varying outcomes: Lazarus effect (complete or almost recovery) Light to moderate disability Moderate to severe disability Where You Can Make a Difference! HERE`S WHERE YOU CAN REALLY MAKE A DIFFERENCE!
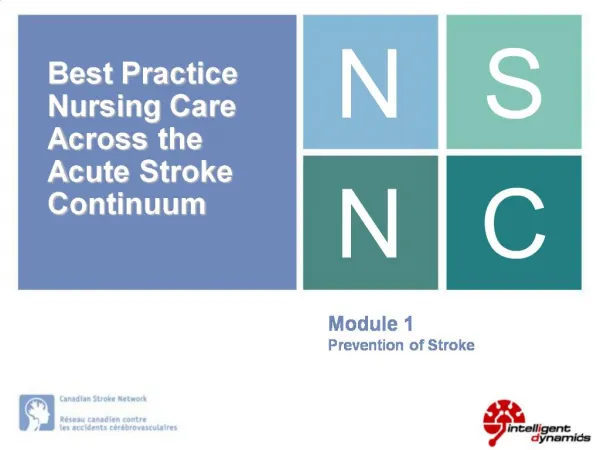
Diminishing Returns over Time ~4h 40min Favorable Outcome (mRS 0-1, BI 95-100, NIHH 0-1) at Day 90 Adjusted odds ratio with 95% confidence interval by stroke onset to treatment time (OTT) ITT population (N=2776) Pooled Analysis NINDS tPA, ATLANTIS, ECASS-I, Courtesy Brott T et al
Hyperacute Stroke Management Your Role in the Emergency Room At your tables, discuss and flip chart key points about your role in the ER: What can you do to assess patients & triage rapidly? What are the key activities of the stroke team? What is your role in facilitating a smooth transfer from ER to an inpatient unit? When done, we’ll debrief the whole group to arrive at some best practices In the Emergency Room TABLE ACTIVITY
Hyperacute Stroke Management What is the single most important key to stroke care success? In the Emergency Room Interprofessional Communication! … so that everyone knows what to do and things can be activated simultaneously!
Hyperacute Stroke Management What needs to get done? In the Emergency Room TABLE ACTIVITY
Hyperacute Stroke Management Include: Maintaining or improving breathing, CV function, nutrition, hydration and electrolyte balance Evidenced based neurological assessment Limiting further neurological damage Preventing complications Treating or modifying reversible risk factors Patient and family education Treatment Objectives
Hyperacute Stroke Management Check airway, breathing, vitals (including temperature) Ensure adequate respiration, monitor BP and cardiac rhythm Establish time of stroke symptom onset Alert “stroke team” Establish IV access-possibly 2 lines Draw blood for CBC, blood glucose and other tests (INR) Early Management – Initial Steps
Hyperacute Stroke Management Perform neuro assessment NIH Stroke Scale Canadian Neurological Scale Use of preprinted standard orders or protocols Order a CT scan Keep NPO until swallowing screen completed Educate patient and family Early Management – Initial Steps
Candidates for t-PA Hyperacute Stroke Management In the Emergency Room
Hyperacute Stroke Management Bypass and repatriation protocols to closest Regional Stroke Centre Established thrombolysis protocol Triage: Rapid assessment using Acute Stroke protocol eligibility criteria / NIH Stroke Scale t-PA target times: ensure you can meet the < 4.5 hr window (ECASS III) Access to CT scanning Stroke team: (Stroke expert, emergency or family physician, nursing staff, allied healthcare professionals, stroke survivor, family, support network central to team) Optimal Stroke Management with rt-PA
Exclusions for t-PA Hyperacute Stroke Management In the Emergency Room