Download
1 / 16
200 likes | 477 Views
Royal College of Physicians of Edinburgh Scottish Stroke Collaboration Meeting 22 nd September 2010 Queen Mother Conference Centre. The Hyperacute Stroke Unit Model NHS Ayrshire & Arran. BACKGROUND 2008. NHS Ayrshire & Arran offers a comprehensive stroke care service.

E N D
Royal College of Physicians of EdinburghScottish Stroke Collaboration Meeting22nd September 2010Queen Mother Conference Centre
BACKGROUND 2008 • NHS Ayrshire & Arran offers a comprehensive stroke care service. • In Ayr hospital - 15 acute stroke beds in 30 bedded acute geriatric assessment unit. 20 rehabilitation beds at different site. • In Crosshouse hospital – 21 acute stroke beds in acute geriatric assessment unit. 20 rehabilitation beds at different site.
QIS Standards 2008 • 70% of stroke patients are admitted within 1 day of admission. • Swallowing assessment 100% on day of admission. • CT scan 80% within 2 days of admission. • Aspirin – 100% of definite ischaemic events within 2 days of admission.
Ayr Hospital 2008 figures • 71% entered stroke unit within 1 day. • Swallowing assessment 64%. • 74% of patients scanned within 2 days of admission. • Aspirin 49% within 1 day.
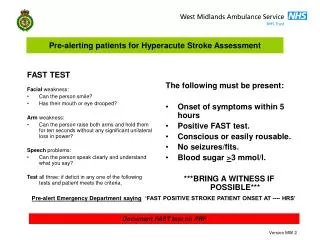
Background of Hyperacute stroke unit (HASU) • Agreed all possible stroke patients should be admitted to a designated area with specialised medical & nursing input. • It would enhance implementation of QIS standards. • Facilitate monitoring of patients with a proposed limited thrombolysis service.
Design of HASU • 6 bedded mixed sex area in 30 bedded acute geriatric assessment unit. • Changed 15 stroke beds to 6 HASU beds & 9 acute stroke beds. • 1 registered nurse & 1 NA allocated 24/ 7 plus an additional registered nurse Mon - Fri 0830 -1630. • Daily medical review followed by brief review of investigation on same day.
Design of HASU • Close monitoring of occupancy with agreed protocol of transferring patients out of HASU. • Priority of at least 1 HASU bed 24/7 for proposed thrombolysis. • Continuous monitoring of all patients including thrombolysis patients. • Additional training for nurses.
Patients journey Patients with possible TIA / Stroke Admission to HASU immediate HASU nurse review including NIHSS medical review non-stroke diagnosed - moved out of HASU Stroke diagnosed – stroke protocol initiated.
Period review • 01-04-08 – 31-03-09 pre- HASU • 01-04-09 – 31-03-10 post- HASU
Pre - HASU 419 Post HASU 527 Number of patients
Pre HASU 419 Number of stroke patients 377 Post HASU 527 Number of stroke patients 403 Number of admissions
Benefits • Allows comprehensive assessment of patients presenting with possible diagnosis of stroke/ TIA. • Facilitates implementation of QIS Standards. • Earlier detection of complications. • Reduces length of stay in hospital. • Safer environment for monitoring stroke patients including those receiving thrombolysis. • Increased motivation of staff in area. • All new stroke patients clearly identified in HASU.
Challenges • Increasing turn over of patients through a very specialised area. • Allows many non-stroke patients to be admitted to HASU. • Requires constant vigilance on bed management. • Requires dedicated nurses with specialist knowledge in stroke. • Requires protected job plan for regular medical supervision at a senior level. • May have impact on AHP workload.
Royal College of Physicians of EdinburghScottish Stroke Collaboration Meeting22nd September 2010Queen Mother Conference Centre