Download
1 / 58
580 likes | 743 Views
Organ transplantation in New Zealand: a panacea ?. •Panacea: noun a solution or remedy for all difficulties or diseases. — ORIGIN Greek panakeia , from panakes ‘all-healing. Johan Rosman Renal Physician and CMO WDHB Johan.Rosman@WaitemataDHB.govt.nz. Mechanisms of graft rejection.

E N D
Organ transplantation in New Zealand: a panacea ? •Panacea: noun a solution or remedy for all difficulties or diseases. — ORIGIN Greek panakeia, from panakes ‘all-healing Johan Rosman Renal Physician and CMO WDHB Johan.Rosman@WaitemataDHB.govt.nz
Solid organ transplantation and the treatment of terminal organ failure • Definitions • Solid organs (kidney, liver, heart, lungs): restrictive • Tissue transplantation (eyes, skin, bone, bone marrow, heart valves, tendons):less restrictive The painting in its three parts: • Transplantations’ global history • The current situation • The future
Tissue Donation(all ‘non solid organs’) • tissues include eyes, heart valves, bone, tendons and skin • tissues do NOT need oxygen to remain suitable for transplant – do NOT need to have an active blood supply • can occur following death regardless of whether death was determined by neurological (brain death) or cardiac (heart stops) assessment • almost everyone can be considered for tissue donation after death
History of Transplantation The1st recorded transplants occurred in the 17th century. The 1st successful organ transplant, a kidney, was performed by a team led by Dr. Joseph Murray on December 23, 1954 between identical twin brothers in Boston. Dr. Murray went on to receive the Nobel Prize in Medicine for this accomplishment. • 1682 - bone • 1881 - skin • 1906 - corneal • 1908 - knee joint • 1954 - kidney transplant • 1966 - pancreas transplant • 1967 - liver transplant • 1967 - heart transplant
Dr. Christian Bernard became a household name when in 1967 he performed the world’s 1st successful heart transplant in Capetown, South Africa.
revolutionized transplantation • increased survival rates • 1st in a new generation of anti-rejection drugs Introduced in 1978, the drug cyclosporine revolutionized transplantation by depressing T cell activation and reducing organ rejection.
Further Successful Firsts in Transplantation • 1981 - heart-lung transplant • 1986 - lung transplant • 1988 - liver/bowel transplant • 1988 - split liver transplant • 1989 - living related liver transplant • 1995 - cluster (liver,bowel,stomach,pancreas & kidney) transplant
Now 22 years post liver transplant, Heather Fisher climbed Mount Kilimanjaro . Transplanted with a liver, bowel, stomach and pancreas at age 5.5 months, Sarah has a spot in the Guiness Book of World Records as the youngest multi-organ recipient. Snowboarder, Chris Klug, won a bronze medal at the 2002 Olympics, two years after his liver transplant. Transplant Successes
Todays’ situation in organ transplantation • There is an increasing number of patients with end organ failure (kidney, liver, heart, lung etc) • There is an increasing demand for organ transplantation • Improvement of technology • Patient expectations • Increase in life expectancy and comorbidities • Diabetes !!!! • There is a finite pool of organs available, even if all potential donors could be used, increasing mismatch demand/supply of organs • Although there is significant progress in the prevention and treatment of acute rejection, hardly any improvement in chronic rejection is made, this limits the long term outlook for transplanted patients
NZ’s Mounting Demographic Pressures Ratio of those aged 65+ to 15-64 0.6 2009 0.5 0.4 Ratio to population aged 15-64 0.3 0.2 0.1 Older (65+) Projection 0.0 1880 1900 1920 1940 1960 1980 2000 2020 2040 2060 2080 2100 Source: Statistics New Zealand
Canadian Transplant Numbers(1994 – 2003) statistics provided by the Canadian Institute for Health Information
Waiting List vs Deceased Donor TransplantsNew Zealand 2004 - 2008 Waiting List * Tx Performed ** Kidneys * Source of Waiting List – NZ Donor Coordinators ** Not included kidneys sent to Australia: 2004 (1) 2005 (4)
Primary Deceased Patient and Graft Survival New Zealand 2002 - 2007 Kidney
Are we getting better at it ?One year patient survival USA(kidney)
Are we getting better at it ? USA Graft Survival (kidney) 1 Year NZ 2008 BUT: hardly any improvement since 1998 !! 2008: NZ 1 year graft survival 94% 5 year graft survival 78 % 5 Year NZ 2008
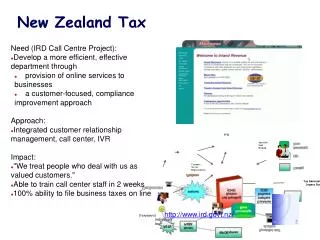
Types of Donation two types of donors: deceased (dead) donors • donor has been declared dead by two physicians independent of the transplant team • usually occurs only in cases of neurologically determined death (the brain stops working 1st but the donor is still on artificial support such as a ventilator to allow the other organs to maintain a blood supply and remain suitable for transplant) live donors • patient chooses to donate one or part of an organ to someone on a transplant waiting list • can only occur with organs when removal will NOT cause grave harm to the donor
Deceased Donation neurologically determined death • usual case • also referred to as brain death • intact heartbeat & circulation • on ventilator • less than 3% of all deaths One the reasons that there are so few organ donors in New Zealand is that very few people die under circumstances that allow them to donate their organs.
Non heart-beating donors donation after cardiac death • currently being explored in New Zealand as the number of classic donors is finite and not sufficient even if used to the max • common in countries such as Spain and the Netherlands • occurs in hopeless cases in the hospital where the decision to withdraw life-support is made (decision is independent of the decision to donate) • organ donation occurs immediately once the heart has stopped and the patient is declared dead • Problem: the treating team is also the team deciding when the patient is formally deceased • Can come with consent issues and sometimes procedures necessary before consent can be obtained
Live Donation • due to more people on the waiting list and a severe shortage of organs for transplant – more emphasis is being put on living donation • kidney – most common • living liver donation on the rise • living lung donation – not as common
usually occurs between related individuals (blood or emotionally) NEVER involves payment to the donor Benefits: can allow for pre-emptive transplant (before recipient requires dialysis) allows for a planned transplant procedure has improved graft survival (often genetic compatibilities and always short time between harvesting and transplantation) shortens time on the waiting list for the recipient increases the total number of organs available for transplant Live Donation
40 years experience with kidneys show no significant long term risks any patient undergoing surgery faces risks – the dilemma with living donation is that a healthy patient is undergoing surgery with no direct health benefit to themselves every attempt is made to minimize risks to the donor informed consent is required Live Donation(risks to the donor ?)
The donor shortage • Optimise recruitment campaign • Use live donors • Use ‘non heart beating donors’ • Use animals • Innovation: ‘pooled live donors’ • Change legislation ? • Improvement in graft survival will have positive impact on demand, improvement in patient survival will not
Legislative approach ? • Sweden and Israel:presumed consent, still donor rates only 15 resp 8 per million • Most succesful: Spain, 34, with opt-out legislation, with however family override,still 10% dies on waiting list • The key to success ?
Other solutions • Allow controlled ‘selling of organs’ • Allow controlled ‘organ tourism’ (unethical for you and me, but for the poor ?) • Improve donorcampaigns ? More transplant coordinators ? • Improve our prevention program, not becoming sick in the first place ?
Problems with live donorshipthe gift of life • Fear • Interfamilial problems (“I want my kidney back”), creating ‘dependency’ • Donor losing his one kidney • Especially in NZ: reimbursement and insurance issues