Download
1 / 25
250 likes | 546 Views
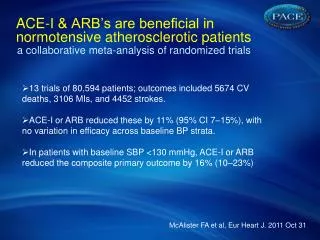
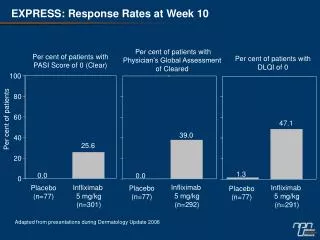
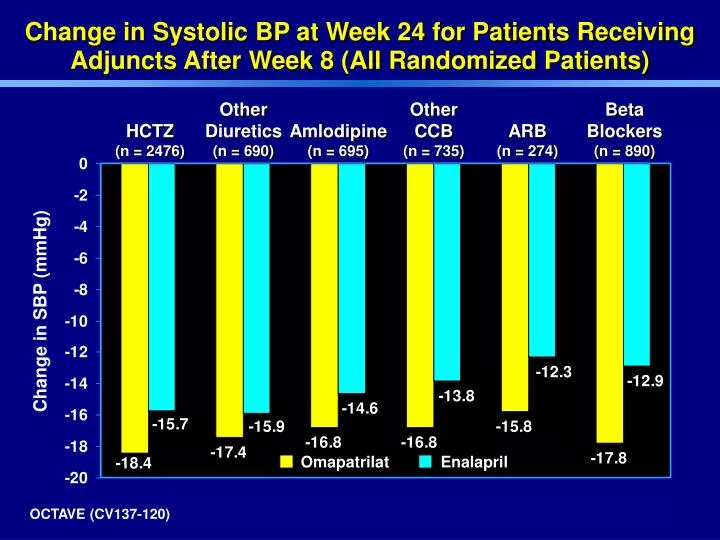
Enalapril. Omapatrilat. Change in Systolic BP at Week 24 for Patients Receiving Adjuncts After Week 8 (All Randomized Patients). Other Diuretics (n = 690). Other CCB (n = 735). Beta Blockers (n = 890). HCTZ (n = 2476). Amlodipine (n = 695). ARB (n = 274). Change in SBP (mmHg).

E N D
Enalapril Omapatrilat Change in Systolic BP at Week 24 for Patients Receiving Adjuncts After Week 8 (All Randomized Patients) Other Diuretics(n = 690) Other CCB(n = 735) Beta Blockers(n = 890) HCTZ(n = 2476) Amlodipine(n = 695) ARB(n = 274) Change in SBP (mmHg) OCTAVE (CV137-120)
Omapatrilat (n = 65) Enalapril (n = 70) OCTAVE Group 3: Effectiveness of Omapatrilatin Patients Treated with HCTZ and Amlodipineat Randomization at Week 24 SBP DBP BP Change (mmHg) OCTAVE (CV137-120)
Enalapril Comparison in Severe Hypertension(CV137-049) B1 B8 B15 B29 B71 20 40 40 80 Forced titrationto 40, elective to 80 Omapatrilat C1 Adjunct Level I Level II Level III SeDBP 115-130mmHg Forced titration to 20, elective to 40 Enalapril 10 20 20 40 A7 B1 B71 C1 Period A Single-Blind Placebo Lead-In Period B Double-Blind Randomized Period C Long-Term Open-Label
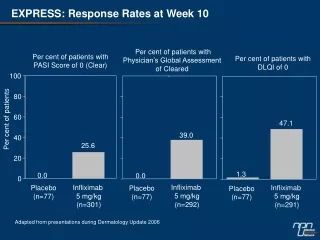
Primary Efficacy ResultsMean Changed from Baseline in Trough SeDBP,and SeSBP and SePP at Week 10 CV137-049
Most Common Adverse Events* * Excluding Angioedema OCTAVE (CV137-120)
Definition of Hospitalization for Heart Failure • OVERTURE Trial • Included all hospitalizations attributable to heart failure as adjudicated by Endpoint Committee which required IV treatmentand had a duration > 24 hours • SOLVD Treatment Trial • Included all hospitalizations attributable to heart failure by the investigator regardless of treatment or duration OVERTURE (CV137-068)
Study Design (CV137-071) Single blind Double blind Placebo Omapatrilat 10 mg 40 mg 80 mg +CAD +Exertional angina R wk 1 wk 2 wk 4 ETT ETT Placebo ETT ETT 3 Wk (max) Period A 4 Wk Period B Day 28 Day 29 BMS data on file
Omapatrilat Placebo Primary Efficacy Results:Change in Peak Exercise Parameters vs Baseline ETT p < 0.001 p < 0.001 p < 0.001 Increased Time (sec) Maximal Exercise Duration Time to Onset of Angina Time to ST Depression BMS data on file CV137-071
Type II diabetics with microalbuminuria (30-300 mg/gram creatinine) or overt nephropathy (> 300 mg/gram creatinine) omapatrilat 20 mg 40 mg 80 mg amlodipine DBP 85-110 mmHg or SeSBP 130-180 mmHg 2.5 mg 5 mg 10 mg wk 4 wk 8 Elective titration Randomization 12 week Double-blind 2 week placebo lead-in Diabetic Patients (CV137-046)
Omapatrilat Amlodipine Summary of Primary Efficacy Results Adjusted Geometric Mean % Change from Baseline for Albumin Excretion Rate Adjusted GM% Change from Baseline Study Week CV137-046
Losartan Comparison in LVH (CV137-038) omapatrilat 20 mg 40 mg 80 mg + HCTZ 80 mg + HCTZ/AML Baseline EchoLVH losartan HypertensionDBP 95-115 mmHgand / orSBP 160-200 mmHg 50 mg 100 mg 100 mg + HCTZ 100 mg + HCTZ/AML Wk 8 Wk 16 Wk 24(Echo) Wk 52(Echo) Force Titration Open-label adjuncts added to Level III
Summary of Primary Efficacy Results Mean Changes from Baseline inEchocardiographic Measures at Week 24 CV137-038
BP Changes From Baseline Per Study Week 0 -5 -10 -15 -20 -25 -30 -35 Losartan Omapatrilat DBP Change in BP (mmHg) SBP 0 24 30 36 44 52 Week Adjunctive therapy % Omapatrilat 6.3 22.2 32.7 32.5 34.4 Losartan 16.5 50.0 54.8 59.3 60.0 CV137-038
CHOIRS Background(Conduit Hemodynamics ofOmapatrilat International Research Study) • Elevated pulse pressure, an indirect measure of increased vascular stiffness, associated with: • Myocardial infarction, stroke • Development and progression of heart failure • Increased mortality • Current epidemic of uncontrolled systolic hypertension due to a lack of treatments thatreduce arterial stiffness • Natriuretic peptides have a favorable effect on largearteries in basic studies although their effects in humans have not been elevated
CHOIRS: Study Design Baseline hemodynamic study (n = 213)SBP 160 mmHg Randomize: Force-titrationWks 0, 2, 4 Enalapril 10 / 20 / 40 mg daily (n = 109) Omapatrilat 10 / 40 / 80 mg daily (n = 104) Withdrawn (n = 22) Withdrawn (n = 24) 8 Wks at maximal dose Trough (24 Hr)Hemodynamic Study (n = 87) Trough (24 Hr)Hemodynamic Study (n = 80)
Central Pulse Pressure (80 ± 20 mmHg) Brachial Pulse Pressure (78.6 ± 16.6 mmHg) 0 -5 -10 -15 -20 0 -5 -10 -15 -20 † * † Enalapril Omapatrilat Central and Peripheral Pulse Pressure * = < 0.005 † = < 0.05 Mitchell, et al., Circulation 2002; 105:2955
Omapatrilat Target Population • Patients with: • A high risk of major cardiovascular events* • Cardiovascular disease (e.g., MI, CHF) • Target organ damage (e.g., LVH, proteinuria) • 3 or more cardiovascular risk factors • Diabetes or renal disease and • Hypertension that is difficult to controlwith existing medications Use with special caution in black patientsand current smokers *Based on WHO-ISH guidelines
Subgroups at Increased CV Risk:Change in Systolic BP at Week 24 Adjusted SBP Changeat Week 24 (mmHg) Omapatrilat Enalapril Difference(oma / ena) Severe Hypertension (n = 7197) Group 1 (n = 983) -18.7 -36.6 -15.9 -32.0 -2.7-4.6 Diabetes Mellitus (n = 3275) -17.6 -13.4 -4.2 Atherosclerotic Disease* (n = 2283) -20.7 -18.0 -2.7 ISH (n = 1332) -22.2 -17.7 -4.5 Renal Disease (n = 582) -17.0 -13.4 -3.6 Heart Failure (n = 233) -20.9 -16.4 -4.5 *Includes chronic stable angina, unstable angina, myocardial infarction, and stroke / TIA OCTAVE (CV137-120)
Omapatrilat Enalapril (n = 2849) (n = 2840) Age (Mean) 62 62 Age, n (%) < 65 years 1654 (58%) 1652 (59%) 65 - 74 years 793 (28%) 802 (28%) ³ 75 years 402 (14%) 385 (14%) Gender, n (%) Male 1602 (56%) 1566 (55%) Female 1247 (44%) 1273 (45%) Race, n (%) White Black 2490 (87%) 314 (11%) 2488 (88%) 309 (11%) Target Population – Baseline Demographics(Diabetes, Renal Disease, Athero Disease, HF) OCTAVE (CV137-120)
Omapatrilat Enalapril OCTAVE: Efficacy in Target Population at Week 24 (Diabetes, Renal Disease, Athero Disease, HF) Use of NewAdjunctive Therapy Change in Systolic BP % of Patients SBP Change (mmHg) ** -3.6** ** p< 0.001 vs enalapril
Target Population – Severity of Angioedema Events, Week 24(Diabetes, Renal Disease, Athero Disease, HF) Number (%) of Patients Omapatrilat (n = 2842) Enalapril (n = 2807) Severity 28 (0.99%) 14 (0.50%) I. No Treatment Administered or Antihistamines Only 15 (0.53%) 2 (0.07%) II. Treated with Catecholamines or Steroids 2 (0.07%) 1 (0.04%) III. Hospitalized but no Mechanical Airway Protection IIIa. No Airway Compromise 2 1 0 0 IIIb. With Airway Compromise 0 (0%) 0 (0%) IV. Mechanical Airway Protection or Death from Airway Compromise 45 (1.58%) 17 (0.61%) Total OCTAVE (CV137-120)
Omapatrilat 80 mg Lisinopril 40 mg Change in 24-Hour Average AmbulatorySystolic BP in Patients Uncontrolledwith ACE-Inhibitor Regimens at Baseline ACE-I Monotherapy(n = 171) ACE-ICombination(n = 75) ASBP Change (mmHg) -11.5** -7.6** Week 4 Maintenance * *p < 0.001 vs. lisinopril CV137-073
Difficult to Control Patients Difficult to Control Patients • Omapatrilat provides consistent benefit in BP reduction over enalapril in each of these difficultto control populations. Untreated patients with severe hypertension Patients uncontrolled witha regimen not including an ACE-I Patients uncontrolled witha regimen including an ACE-I
BP Control in Uncontrolled Patients at Sites with Highest Adjunct Use (64.0% - 100%) at Week 24 Change in SBP (mmHg) BP Control n / N (%) Difference Omapatrilat (n = 967) Enalapril (n = 966) 544 / 907 (60.0%) 466 / 903 (51.6%) -19.1 -15.7 -3.4 OCTAVE (CV137-120)
Retail Pharmacist Validation of Counseling and Delivery of Patient Education Medication Dispensed in Unit-of-Use Packaging Message with PPI Omapatrilat Educational Program Counseling PharmacistEducation MD Education Initial MD-Patient ConsultationPatient BrochureRx Given Mandatory Counseling Service Retail PharmacistEducation Follow-up MD Patient ConsultationRx Given