Download
1 / 20
210 likes | 515 Views
Approaches to the management of adults with acute lymphoblastic leukemia. Dr. Santiago Pavlovsky Scientific Director Angelica Ocampo Hospitalisation and Clinical Research Center - FUNDALEU Buenos Aires - Argentina.

E N D
Approaches to the management of adults with acute lymphoblastic leukemia Dr. Santiago Pavlovsky Scientific Director Angelica Ocampo Hospitalisation and Clinical Research Center - FUNDALEU Buenos Aires - Argentina
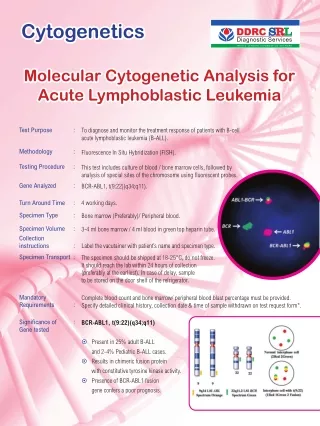
WHO histological classification of precursor B-cell, T cell, and mature B-cell neoplasms • Precursor B lymphoblastic leukemia/lymphoma: 70-85% adults ALL FAB: L1, L2; 10-15% lymphoblastic lymphoma. Phenotype:TdT (+), CD19 (+), CD22 (+), CD20 (+), CD79a+, S Ig (-). Cytogenetic:t (9;22) BCR/ABL (30%), t (4;11) gene ALL1/ AF4 ( 36%) • Precursor T lymphoblastic leukemia/lymphoma: 25% adults ALL FAB: L1, L2; 85-90% Lymphoblastic Lymphoma. Phenotype: CD3 (+), CD4 (+), CD5 (+), CD7 (+), CD8 (+). Cytogenetic: MYC (8q 24.1) • Mature B-cell leukemia/lymphoma: 2-4% adults ALL FAB: L3, CD19 (+), CD20 (+), CD22 (+), TdT (-), S IgM (+), Ki-67 >95% of cells; t (8;14) (q24;q32) oncogene c-MYC. 2-3% are adult Burkitt ´s lymphoma.
Adverse prognostic factors in adults ALL • Time to CR > 4 weeks. Late responders • Age > 35 years old. • Leukocyte > 30.000/mm3 • Immunophenotype: Pro B (B-lin., CD10-) Early T (T-lin., CD1a-, sCD3-) Mature T (T-lin., CD1a-, sCD3+) • Cytogenetics: t (9;22) BCR/ABL t (4;11) ALL1/AF4 • MRD (+) after induction and consolidation positive.
Treatment strategy in the 80`s and 90`s BFM based for adults ALL • Induction: Prednisone-vincristine-daunorubicin- L-asparaginase for four weeks. • Consolidation: High-dose (CPM, Ara-C, Mtx) rotational of brief duration. • G-CSF: Reduce duration of neutropenia and early mortality (4% vs 11%). • CNS prophylaxis: High-dose MTX and TIT (ara-C- MTX-DMT). • Maintenance: 6MP+MTX with pulses for 18-24 mo. • Allo-BMT: For high-risk patients <45 years old.
Results of recents adult ALL trials Group Year No Pts Age %CR %LFS %OSV • GMALL 02/84 1993 562 28 75 39 (7y) 49 • FGTALL 1993 581 33 76 32 (4y) • MRC-UKALL 1997 618 >15 82 29 (5y) 29 • PETHEMA -93 1998 108 28 86 41 (4y) 47 • MRC/ECOG 1999 920 -- 89 • MDACC 2000 204 39 91 38 (5y) 39(5y) • GMALL 05/93 2001 1163 35 83 44(3y) 47(3y) • GIMENA 0288 2002 794 28 82 33 (9y) 27 (9y) • LALA-94 2004 922 33 84 30 (5y) 33 (5y) • CALGB 19802 2005 163 40 79 32 (3y) 36 (3y) • Total 6035 75-91 34 (5y) 36 (5y)
Results of therapy in adults ALL according to GATLA protocols Trial Years Consol No Pts %CR %DFS %OSV 5 years 1/79 to 2/82 No 135 80 15 1 24 2 3/82 to 6/87 Yes 144 79 30 38 7/87 to 7/00 Yes 190 80 36 43 8/00 to 8/05 Yes 100 80 30 (4y) 36 (4y) 1: P=0.004 2: P=0.005 Lluesma-Goñalons M, Pavlovsky S, et al: Ann Oncol 2:33-39,1991
EFS in favourable risk (WBC < 30,000/mm3 and age < 35 years) in adults ALL. GATLA P<0.001 48% 45% 18% Months
EFS in unfauvorable risk according to protocol in adults ALL. GATLA 1979 to 2005 P=0.290 25% 19% 13% Months
Pediatric vs adults therapeutic trials in adolescent (15-21 ys) with ALL Protocol Country Type No pts %CR %EFS FRALLE-93 France1 Pediatr 77 94 67 LALA-94 Adults 100 83 41 CCG USA2 Pediatr 196 96 64 CALGB Adults 103 93 38 • Boissel N et al: J Clin Oncol 21:774-780,2003 • Stock W, et al: Blood 96:476a,suppl,2000
A randomized controled trial of filgastrin (G-CSF) during induction and consolidation therapy for 198 adults ALL. CALGB 91111 G-CSF Placebo P Induction: PMN >1000/mm3 days 16 22 <0.001 Hospital days 22 28 =0.02 Consolidation: PMN >1000/mm3 days 6 9 Median DFS (ys) 2.3 1.7 =0.53 Median OSV (ys) 2.4 1.8 =0.25 Conclusion: G-CSF improve neutrophil recovery but not affect the outcome. RA Larson et al: Blood 92:1556-1564,1998
Comparison of chemotherapy versus Allo-BMT for adults ALL in first complete remission. • Therapy Chemo Allo-BMT P< • Source GALLSG IBMTR • No Centers 44 98 • No Pts 484 234 • % Relapses 9 ys 66 30 0.0001 • % LFS 9 ys 32 34 0.02 Zhang MJ et al: Ann Intern Med 123:428-431,1995
Allo versus auto transplantation in adults ALL. A GOELAMS trial. • Eligible 198 pts, median age 33 yrs, CR rate 86% • Transplant Allo Auto P= • No Pts (<50 ys) 41 106 • TRM at 6 mo 15% 3% • DFS at 6 ys 75% 33% 0.0004 • OSV at 6 ys 75% 40% 0.0027 M Hunault et al: Blood 104:3028-3037,2004
Comparison of intensive chemo, Allo or Auto SCT as post-remision Tx for adults with high-risk ALL. PETHEMA ALL-93 trial High-risk: age 30-50 ys or WBC>25x109/L or t(9;22, t(4;14) Eligible: 222 pts, CR 183 pts (82%), 5 ys DFS: 35%,OSV 34% Chemo AlloSCT AutoSCT P= No/Rand 36/48 57/84 31/50 %relapse 46 62 57 N.S. %DFS 5 ys 44 35 33 N.S. %OSV 5 ys 50 35 37 N.S. JM Ribera et al. Haematol 90:1346-1356,2005
Therapy for Mature B-cell adults ALL Protocol Center No Pts %CR %LFS %SV 5ys Ref B-NHL83 * GALLSG 24 63 50 49 1 B-NHL86 * GALLSG 35 74 71 51 1 Prot 9251 CALGB 24 75 66 52 2 Hyper-CVAD MDACC 26 81 61 49 3 Hyp-CVAD-R MDACC 31 86 88 89 4 • Short intensive therapy with six short alternately cycles A and B with high-dose MTX, CPM, or Ifosfamide, VM26 and Ara-C plus TIT. 1) Hoelzer D et al: Blood 87:495-508,1996 2) Lee EJ, et al: J Clin Oncol 19:4014-4022,2001 3) Thomas DA et al: J Clin Oncol 17:2461,1999 4) Thomas DA et al. Blood 106:47a,Abstr 149,2005
Historical comparison of Imatinib plus chemo (I-C) vs chemo (C) only preceding stem cell transplantation in newly diagnosed Ph´+ ALL • Pre-SCT therapy Chemo Chemo+Imatinib P • No Pts 31 29 • % CR 82 79 NS • % relapse prior SCT 42 3.5 =0.002 • % DFS 38 76 =0.001 Seok L et al. Blood 104:Abstr 2740,2004
Outcome in naive adults BCR-ABL + ALL treated with Imatinib plus intensive chemotherapy. • Therapy MDACC1 JALSG2 UKALL3 GRA ALL4 • No Patients 35 80 27 29 • % CHR 94 96 89 69 % C Mol R 24 78 • No BMT 13 (36%) 15 (63%) 15 (56%) • DFS 78% (3ys) 45% (2yr) 56% (1yr) 57% (1yr) • OSV 58% (2yr) 59% (1yr) 71% (1yr) • Historical DFS after BMT without Imatinib: 30-40% 1) DA Thomas et al. Blood 106:520a,Abstr 1830,2005 2) M Janada et al. Blood 106:Abstr 1827,2005 3) B Patel B et al. Blood 106:523a,Abstr 1839,2005 4) A Delannoy et al. Blood 106: Abstr 146,2005 (Pts >54 ys)
Imatinib given concurrenttly versus subsequent to induction and consolidation in newly diagnosis adults Ph`+ ALL • Imatinib 600 mg subsequent concurrent • No patients 48 46 • Log reduction 1.5 log 3.9 log • BCR/ABL neg PCR 10% 50% • % CR 96% • Grade III-IV toxicity lower higher OG Ottmann et al. Blood 104;No 11,abstr 685,2004
Facts of Imatinib in BCR-ABL positive adults ALL • In 56 relapse/refractory patients Imatinib alone produced a 60% ORR with 19% CR. The TTP and OSV was 2.2 and 4.9 months respectively. (OG Ottmann et al: Blood 100:1965,2002) • Imatinib not cross the blood brain barrier and has a significant risk of CNS relapse without CNS prophylaxis. • Daily dose of Imatinib should be 600-800 mg. • As first line imatinib plus chemo produce 85-95% of CR. • Concurrent Imatinib /chemo is clearly superior than sequential or alternating, based on Q-RT-PCR determinations of BCR-ABL transcript levels.
Target therapy in association with chemotherapy according to phenotype and BCR-ABL in adults ALL. Phenotype BCR-ABL CD20 CD52 Therapy T-Precursor Negative Negat. >10%+ Chemo+Alentuz Positive Negat. Negat. Chemo+Imatinib B-Precursor Posit. Negat. Chemo+Ritux. Negative Negat. Negat. Chemo only Negat. >10%+ Chemo+Alentuz Mature B Negative Posit. Chemo+Ritux.
Conclusions • The largest advances in treatment of adults ALL were derived from the introduction of multiagent BFM like regimen on induction, consolidation and maintenance. • The ALL strategy must be perform according to cytological classification Precursor B or T cells or B mature cells . • MRD-based early response by flow cytometry or immunoglobulin H gene analysis identify the majority of patients at risk to relapse, and safe others from inadequately toxic therapy. • The use of Imatinib with chemo on induction and consolidation improve the prognosis of BCR/ABL positive adult ALL.