Download
1 / 75
750 likes | 854 Views
A baby with cloverleaf skull anomaly. R 3 羅永邦 Supervisors: Drs. 許瓊心 , 林炫沛 & 邱南昌. Admission Data. Name: 黃 xx 之女 ( 張 xx) Number: 3619275-6 Sex: Female Admission Date: 94/05/30 Chief complaints: 1. Prematurity (GA: 32 weeks) 2. Respiratory distress 3. Congenital anomaly.

E N D
A baby with cloverleaf skull anomaly R 3 羅永邦 Supervisors: Drs. 許瓊心, 林炫沛 & 邱南昌
Admission Data • Name: 黃xx之女 (張xx) • Number: 3619275-6 • Sex: Female • Admission Date: 94/05/30 • Chief complaints: 1. Prematurity (GA: 32 weeks) 2. Respiratory distress 3. Congenital anomaly
Present Illness • Perinatal examinations at OBS/GYN Clinic did not show any abnormality. • Mother was also denied of perinatal drug usage, infection or systemic disease. • PROM was noted since 5/12 and tocolysis performed since 5/12 at OBS/GYN Clinic. Ampicillin Tx from 5/12 and 2 doses of Decadron were given.
Present Illness • Due to fetal distress (HR: 80-90/min), emergency C/S was performed. The Apgar score 71 95. • After birth, bradycardia was noted and endotracheal tube was inserted. Under the diagnosis of PPROM, prematurity and respiratory distress, she was admitted for further treatment and evaluation.
Present Illness • Birth history: DOB on 94/05/30 at 22:26 EDC: 94/07/20 GA: 32+ weeks, BBW: 1,910gm Via C/S due to fetal distress Apgar score: 7195 PPROM noted since 05/12 Prenatal ampicillin since 05/12 Prenatal steroid x2 doses
Present Illness • Maternal history G1P1 healthy mother No GDM, HTN, Toxemia, APH, PPH URI(-), Fever(-) HBsAg(-), HBeAg(-)
Family History 28 years old BG: AB 電子業 34 years old BG: AB 電子業
Physical Examination • Blood pressure: 56/3744/29Dopamine used58/36 • Heart rate: 116 /min • Respiratory rate: 60 /min • Body temperature: 36.3C • General appearance: acute ill looking
Physical Examination Eyes: not injected Ear: suspect ear canal obstruction Nose: suspect left canal Obstruction Mouth: no cleft palate Head: Cloverleaf skull Frontal bone bossing Anterior fontanel: 7.5 x 4.5cm Mid-face hypoplasia
Physical Examination Frontal area bossing Pseudo low set ears Exophthalmos
Physical Examination Thorax: symmetric expansion no pigeon chest Chest: breathing sound: coarse No rale, no wheezing Heart: RHB, no murmur or thrill Abdomen: Soft and flat Bowel sound: normactive No hepatosplenomegaly Extremities: free movable No shortened limbs Rectum and anus: patent
Laboratory Data (5/30) • CXR (5/30): Parahilar radiating congestion of both lungs is seen. Slight overaeration of bilateral lungs is seen. • No limbs or vertebrae abnormalities • IMP: Retention of lung fluid.
Impression • 1. Prematurity (GA: 32+ weeks, BBW: 1910 gm) • 2. PROM about 18 days • 3. Respiratory distress, suspect RDS grade I • 4. Hypotension • 5. Congenital anomaly r/o Crouzon syndrome r/o Thanatophoric dysplasia r/o Craniosynostosis
Hospital Course • Initial management: 1. On ETT + IMV 2. N/S challenge first, then add Dopamine (5/30~5/31) 3. Ampicillin and gentamicin (5/30~6/06) for suspected congenital infection
Hospital Course • Brain echo (5/31): Ventricular dilatation, bilateral; suspect pachygyria • Renal echo (5/31): negative findings • Abdominal echo (5/31): gall bladder is visible; no intra-abdominal mass was noted • Heart echo (5/31): PDA (left to right, 0.146 cm), PHT (56.5 mmHg), Dysarrhythmia
Hospital Course • His respiratory distress improved, so endotracheal tube was removed and changed to O2 hood since 6/01 • DC O2 hood on 6/07
Skull PA + LAT view (6/01) Obliteration of bilateral coronal and Lambdoidal sutures of skull is seen. Premature closure is considered. Association with cloverleaf skull syndrome is considered
Hospital Course • Consult Ophthalmologist: Incomplete regression of hyaloid vessels; Vessels constriction of left eye Impression: 1. Congenital abnormality of retinal vessel (OS) 2. Optic neuropathy (OS) Suggest VEP examinations after general condition stabilized
Hospital Course • Add aminophylline since 6/02 • F/U brain echo (6/03): Ventriculomegaly, bilateral, symmetric; Suspect pachygyria; High RI (0.94) • Arrange brain MRI with/without contrast on 6/03
1. Dilatation of the lateral ventricles is noted, The 3rd ventricle is mildly dilated. Presence of cavum septum pellucidum and cavum vergae is noted. 2. The cerebral cortical sulci is broad and flattened, pachygyria is considered. 3. Brachicephaly is noted. Trilobed skull is demonstrated on coronal images. Cloverleaf skull syndrome due to premature closure of multiple cranial sutures is considered. 4. The posterior portion of the septum pellucidum is not visualized. 94.6.3 Cavum septum pellucidum Cavum vergae
1. The posterior fossa Is small and torcular is low Lying. Tonsillar herniation Thru the foramen magnum Is also noted. 2. No abnormal enhancement is noted. 3. The pituitary gland, cavernous sinuses and cerebellopontine angles appear normal and symmetric.
Brain MRI (6/03) • Impression: 1. Cloverleaf skull syndrome, following anomalies including acrocephalopolysyndactylies (Crouzon, Pfeiffer, Carpenter, Apert…etc.) and type II form of thanatophoric dysplasia should be considered in the differential diagnosis. 2. Dilatation of the lateral ventricles and presence of cavum septum pellucidum and cavum vergae. 3. Pachygyria. 4. Small posterior fossa and cerebellar tonsilar herniation. 5. Absent posterior septum pellucidum.
Brain CT (6/09) 1. Dilatation of the lateral ventricles and mild dilatation of the 3rd ventricle are noted. Presence of cavum septum pellucidum and cavum vergae is noted. 2. The posterior septum pellucidum is not visualized.
Brain CT (6/09) 1. Premature closure of multiple cranial sutures causing trilobed appearance of skull on coronal images and brachicephaly is seen, cloverleaf skull syndrome is considered. Beaten copper appearance of the skull is also noted. 2. Enlargement of the fontanelles is noted.
Brain CT (6/09) • Impression: 1. Cloverleaf skull syndrome. 2. Dilatation of the lateral ventricles and mild dilatation of the 3rd ventricle and presence of cavum septum pellucidum and cavum vergae. 3. Absent posterior septum pellucidum.
Hospital Course • Frequent bradycardia (70~80/min), apnea and desaturation (70~80%) noted on 6/15 • No fever, no hypotension • Head circumference increased from 27.5 cm to 29 cm • Brain echo (6/15): Progressing ventriculomegaly, bilateral Hydrocephalus, non-communicating type Pachygyria, suspect lissencephaly High RI (1.0)
Hospital Course • IICP was highly suspected, so CSF tapping was performed, however, reddish CSF fluid was noted • Lab data (1) • Lab data (2) • CXR • Brain CT (6/15): 1. Cloverleaf skull syndrome. 2. Dilatation of the lateral ventricles and mild dilatation of the 3rd ventricle and presence of cavum septum pellucidum and cavum vergae. 3. Absent posterior septum pellucidum.
Hospital Course • Consult Neurosurgeon immediately • Extraventricular device was inserted on 6/15, then Cefamezine for post-operation prophylaxis (6/16~6/18) • PRBC was transfused after OP • Luminal for preventing seizure (6/15~)
Hospital Course • Her bradycardia and desaturation improved a lot after operation • EVD discharge: 18cc (6/16)37cc (6/17) 22.5cc (6/18)24cc (6/19) • Brain echo (6/16): Hydrocephalus, /p V-P shunt; Decreased ventricle size, bilateral
Hospital Course • Unfortunately, her FGFR3 gene PCR showed positive on 6/18, so Thanatophoric dysplasia was highly suspected • Very poor prognosis was told, so her family decided to remove EVD shunt since then • After detailed explanation of the consequence of removing EVD shunt to her family, her EVD shunt was removed on 6/24
Hospital Course • However, further genetic study had ruled out the possibility of thanatophoric dysplasia Newborn screen: normal Tandem mass: normal Sequencing of FGFR3 gene: normal PCR study of FGFR2 gene: pending
Hospital Course • Brain echo (6/30): 1. Progressive bilateral ventricle dilatation 2. Suspect blood clot inside the ventricle, bilateral 3. Porencephaly at right fronto-parietal area, due to EVD 4. High RI (0.97) • Brain echo (7/06): 1. Hydrocephalus, non-communicating type, progressing 2. Porencephaly at right fronto-parietal area, progressing 3. High RI (1.0)
Hospital Course (7/07) • At this point, she would get bradycardia easily if you press on her anterior fontanel gently
Hospital Course • This patient was discharged on 7/16 • However, she was brought back to our ER on 7/18 without breathing & heart beating • Unfortunately, she died on 7/18
Discussion Craniosynostosis Cloverleaf skull syndrome
Craniosynostosis • Primary craniosynostosis: a primary defect of ossification • Secondary craniosynostosis: a failure of brain growth, more commonly • Syndromic craniosynostosis: display other body deformities
Craniosynostosis • Simple craniosynostosis: only 1 suture fuses prematurely • Complex or compound craniosynostosis: premature fusion of multiple sutures
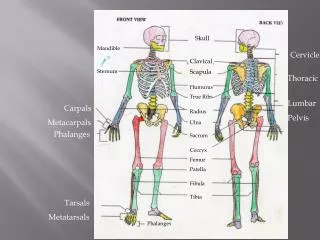
Craniosynostosis • The coronal suture separates the 2 frontal bones from the parietal bones. • The metopic suture separates the frontal bones. • The sagittal suture separates the 2 parietal bones. • The lambdoid suture separates the occipital bone from the 2 parietal bones. • The primary factor that keeps sutures open is ongoing brain growth. • Normal skull growth occurs perpendicular to each suture.
Primary craniosynostosis • When 1 or more sutures fuse prematurely, skull growth can be restricted perpendicular to the suture. If multiple sutures fuse while the brain is still increasing in size, intracranial pressure can increase. • Cause: a primary defect in the mesenchymal layer ossification in the cranial bones. • A gene locus for single suture craniosynostosis has not been identified.
Ant. plagiocephaly - Early fusion of 1 coronal suturePost. plagiocephaly - Early closure of 1 lambdoid suture