Download
1 / 18
180 likes | 470 Views
AAA and PVD. Emily Pallister and Sanjena Mithra. The plan…. Cases Basic facts you probably already know! Finals style tasks. Objectives. To demonstrate common clinical presentations of PVD and AAA

E N D
AAA and PVD Emily Pallister and SanjenaMithra
The plan… • Cases • Basic facts you probably already know! • Finals style tasks
Objectives • To demonstrate common clinical presentations of PVD and AAA • To revisit incidence, pathogenesis and management of PVD (Arterial and Venous, Ulcers) and AAA • To revise the difference between acute and chronic limb ischaemia • To consider approach to these cases in finals
Case 1 • 80 yo gentleman sent by GP to A&E. Had been investigated for right hip pain. Xray of right hip demonstrated no hip injury but GP noted calcified aneurysmal aorta. • PMH: Hypertension
Questions… • Is this a typical presentation? • How would you investigate/manage this patient?
Investigations and Management Management: • History and examination • Bloods incl FBC, UE, G&S • Investigations – USS/CT • ECG • Consider CPEX and ECHO • EVAR/Open Repair
Aneurysms • Definition: Permanent dilation of artery to 2x normal diameter • True Aneurysm: All layers of arterial wall involved Due to degeneration of elastic lamina and SM loss • False Aneurysm: Blood collects around vessel wall communicating with lumen. Surrounding tissues form wall of aneurysm.
Some facts about AAA! • 5% incidence over 60 y.o. Increases with age. • 5M:1F • Risk of rupture <1%/yr when AAA <5.5cm 25%/yr when AAA >6cm Symptoms: Usually asymptomatic except when impending rupture – Severe epigastric pain radiating to back. HR BP Hb
Peripheral Arterial Disease • Mild ischaemia • Cramping pain • Calf/thigh/buttock • Fixed claudication distance • ABPI 0.9-0.6 • Severe ischaemia • Burning pain in foot • Shorter distance • No tissue loss • Worse at night • ABPI 0.6-0.3 • Severe ischaemia + tissue loss • Gangrene • Whole limb threatened • Painful, cold, numb • ABPI <0.3
Case 2 45 yo gentleman admitted via A&E with dry necrotic right hallux. • What else do you want to know about this patient?
Case 2 cont’d On examination the gentleman has a pale, cold right leg with no distal pulses felt. He has no tissue loss. He reports long standing rest pain and is suffering a lot of pain currently. He has extensive smoking history but is not diabetic. • What will your initial investigations/management be? • How would you stage his PVD?
Task You decide that this patient would benefit from an angiogram. Explain the procedure to the patient and consent for the process.
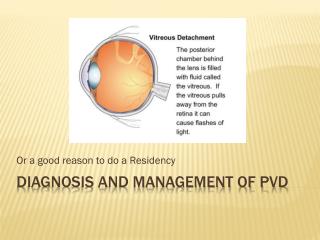
Peripheral Venous Disease • Due to valvular incompetence or damage to veins. • Blood can’t drain from capillaries. Irritates skin -> impairs 02 exchange -> tissue breakdown and fibrosis
Case 3 87 yo lady referred in from district nurses with extensive bilateral ulcers, worse on the right. • What questions do you want to ask us regarding the ulcers?
Ulcers • Complete loss of epidermis and part of dermis • Affects 2% population