Download
1 / 40
510 likes | 2.01k Views
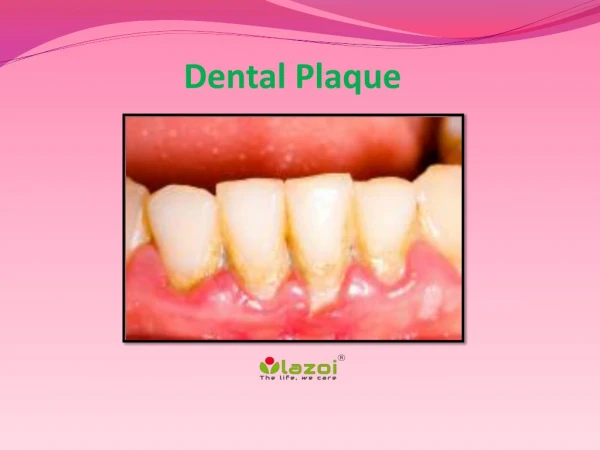
Dental Plaque. Definitions. According to Bowden, Dental plaque can be defined as the soft tissue deposits that form the biofilm adhering to the tooth surface or on the other hard surfaces in the oral cavity, including removable and fixed restorations.

E N D
Definitions • According to Bowden, Dental plaque can be defined as the soft tissue deposits that form the biofilm adhering to the tooth surface or on the other hard surfaces in the oral cavity, including removable and fixed restorations. • According to Marsh, Dental plaque can be defined as the diverse community of microorganisms found on the tooth surface as a biofilm, embedded in an extracellular matrix of polymers of host and microbial origin.
Dental plaque must be differentiated from other tooth deposits, like materia alba and calculus. • Materia Alba refers to soft accumulations of bacteria and tissue cells that lack the organized structure of dental plaque. • Calculus is hard deposits that form by mineralization of dental plaque and is generally covered by a layer of unmineralised plaque.
Plaque • Plaque can be defined as a complex microbial community, with greater than 1010 bacteria per milligram. It has been estimated that as many as 400 distinct bacterial species may be found in plaque. • In addition to the bacterial cells, plaque contains a small number of epithelial cells, leukocytes, and macrophages. The cells are contained within an extracellular matrix, which is formed from bacterial products and saliva. • The extracellular matrix contains protein, polysaccharide, lipids and glycoproteins
Inorganic components are also found in dental plaque; largely calcium and phosphorus which are primarily derived from saliva. • The inorganic content of plaque is greatly increased with the development of calculus. • The process of calculus formation involves the calcification of dental plaque. • The practical consequences of calculus formation are that the deposit is significantly more difficult to remove once calcified, and it leaves a rough surface on the root which is easily colonized by plaque..
Dental plaque can be classified in several different ways. • Plaque is classified as supragingival or subgingival based on its relationship to the gingival margin. Supragingival plaque is evident on the tooth above the gingival margin • Plaque can also be classified by its relationship to the tooth surface, as either attached or unattached plaque. • The unattached subgingival plaque is more closely associated with the wall of the subgingival tissues than is the attached plaque. • Lastly, plaque has been classified by association with disease state as "health-associated" or "disease-associated". The latter classification is related to differences in the microbial composition of dental plaque in health versus disease.
Development of dental plaque • The development of dental plaque has been studied in humans as well as non-human animal model systems. • One of the most commonly used models of plaque development is referred to as the "experimental gingivitis" model (Loe, et al., 1965). • This protocol involves the examination of subjects (usually dental students!) who abstain from any oral hygiene measures for a period of three weeks. • These studies have provided much information on the structural and microbiological characteristics of dental plaque.
The pellicle is evident as lightly stained material on a tooth surface when patients use disclosing solution. • A newly cleaned tooth surface is rapidly covered with a glycoprotein deposit referred to as "pellicle". • The pellicle is derived from salivary constituents which are selectively adsorbed onto the tooth surface. • Components of the dental pellicle include albumin, lysozyme, amylase, immunoglobulin A, proline-rich proteins and mucins. • The formation of pellicle is the first step in plaque formation.
The pellicle-coated tooth surface is colonized by Gram-positive bacteria such as Streptococcus sanguis, Streptococcus mutans, and Actinomyces viscosus. These organisms are examples of the "primary colonizers" of dental plaque. • Bacterial surface molecules interact with components of the dental pellicle to enable the bacteria to attach or adhere to the pellicle-coated tooth surface. • For example, specific protein molecules found as part of the bacterial fimbria (hair-like protein extensions from the bacterial cell surface) on both Streptococcus sanguis and Actinomyces viscosus interact with specific proteins of the pellicle (the proline-rich proteins) with a "lock and key" mechanism that results in the bacteria firmly sticking to the pellicle-coating on the tooth surface (Mergenhagen et al. 1987). • Within a short time after cleaning a tooth, these Gram-positive species may be found on the tooth surface.
After the initial colonization of the tooth surface, plaque increases by two distinct mechanisms: • the multiplication of bacteria already attached to the tooth surface, and • the subsequent attachment and multiplication of new bacterial species to cells of bacteria already present in the plaque mass. The secondary colonizers include Gram-negative species such as Fusobacterium nucleatum, Prevotella intermedia, and Capnocytophaga species. A key property of these microorganisms appears to be the ability to adhere to Gram-positive species already present in the existing plaque mass. These organisms would typically be found in plaque after 1 to 3 days of accumulation.
After one week of plaque accumulation, other Gram-negative species may also be present in plaque. These species represent what is considered to be the "tertiary colonizers", and include Porphyromonas gingivalis, Campylobacter rectus, Eikenella corrodens, Actinobacillus actinomycetemcomitans, and the oral spirochetes (Treponema species). • The structural characteristics of dental plaque in this time period reveal complex patterns of bacterial cells of cocci, rods, fusiform, filaments, and spirochetes. In particular, specific associations of different bacterial forms have been observed.
The structural interactions of the bacteria probably are a reflection of the complex metabolic interactions that are known to occur between different plaque microorganisms. • One example of this is the production of succinic acid from Campylobacter species that is known to be used as a growth factor by Porphyromonas gingivalis. Streptococcus and Actinomyces species produce formate, which may then be used by Campylobacter species. • Fusobacterium species produce both thiamine and isobutyrate that may be used by spirochetes to support their growth. • The metabolic and structural interactions between different plaque microorganisms are a reflection of the incredible complexity of this ecological niche.
Plaque in health and disease • The overall pattern observed in dental plaque development is a very characteristic shift from the early predominance of Gram-positive facultative microorganisms to the later predominance of Gram-negative anaerobic microorganisms, as the plaque mass accumulates and matures. • This developmental progression is also reflected in the shifts in predominant microorganisms that are observed in the transition from health to disease. • Studies of plaque taken from sites of health or disease and examined either microscopically or by culturing have demonstrated distinct differences in health versus disease-associated microbial populations.
Microscopic studies of plaque have examined the presence of different morphological types ("morphotypes") of bacteria. • studies reveal an increase in the presence of motile rods and spirochetal organisms in gingivitis and periodontitis as compared to gingival health. • A major limitation of studies of bacterial morphotypes is that many "health-associated" microorganisms are indistinguishable from "disease-associated" microorganisms (for example, Streptococcus species and Porphyromonas gingivalis, respectively). • However, cultural studies also reveal characteristic distinctions between health- and disease-associated plaque.
The percentage of Gram-positive rods and cocci decrease in gingivitis- and periodontitis-associated plaque as compared to health-associated plaque. • Similarly, the percentage of microbiota comprised of Gram-negative anaerobic species is greatly increased in gingivitis (approximately 25%) and periodontitis (approximately 75%) as compared to health (approximately 13%, Slots, 1979). • Specific microbial species that are important in plaque development and disease development are outlined below based on their categorization by cell wall morphology (Gram-positive, Gram-negative, or spirochetal) and their physiological status (facultative or anaerobic).
SELECTED BACTERIAL SPECIES FOUND IN DENTAL PLAQUE Facultative Anaerobic Gram-Positive • Streptococcus mutans • Streptococcus sanguis • Actinomyces viscosus Gram-negative • Actinobacillus actinomycetemcomitans • Capnocytophypa species • Eikenella corrodens • Porphyromonas gingivalis • Fusobacterium nucleatum • Prevotella intermedia • Bacteroides forsythus • Campylobacter rectus • Spirochetes • Treponema denticola • (Other Treponema species)
Relationship of Specific Microorganisms to Periodontal Diseases • Our understanding of the relationship between the microorganisms found in dental plaque and the common dental disease of periodontitis has undergone numerous phases historically • Early in the 19th century, it was felt that, like the situation with diseases such as tuberculosis, a specific bacterial species was responsible for the disease processes. • The criteria by which a given bacterial species was associated with disease historically has been through the application of Koch's Postulates.
These criteria were developed by Robert Koch in the late 1800's. The criteria are as follows: • A specific organism can always be found in association with a given disease. • The organism can be isolated and grown in pure culture in the laboratory. • The pure culture will produce the disease when inoculated into a susceptible animal. • It is possible to recover the organism in pure culture from the experimentally infected animal.
Non-Specific Plaque Hypothesis (Loesche,1976) • However, the concept that a specific bacterial species was responsible for periodontal diseases fell out of favor for several reasons. First, despite numerous attempts, a specific bacterial agent was not isolated from diseased individuals. Rather, the organisms found associated with disease were also found associated with health. • Good experimental animal model systems of periodontal disease were not available to test the pathogenicity of specific microorganisms (this, in fact, remains problematic today).
Further, in the mid 1900's, epidemiological studies indicated that the older an individual was, the more likely they were to have periodontal disease. This led to the concept that the bacterial plaque itself, irrespective of the specific bacteria found in plaque, was associated with disease. This concept, known as the Non-Specific Plaque Hypothesis (Loesche, 1976), held that all bacteria were equally effective in causing disease.
Specific Plaque Hypothesis (Loesche,1976 • Several important developments caused a change in this thinking. • First, it was realized that organisms that are found as part of the "normal" bacterial flora (i.e., found in health), may function as pathogens under certain conditions. These organisms may be altered, or increase significantly in numbers relative to other non-pathogenic species, to function as pathogens. • This type of bacterial pathogen is referred to as an endogenous pathogen, in contrast to an organism that is not normally found in healthy states which is termed an exogenous pathogen.
Secondly, tremendous advances were made in the 1960's and 1970's in techniques used to culture anaerobic microorganisms (bacterial species that cannot grow in the presence of oxygen). • These advances were related to the anaerobic culturing conditions as well as the nutrients required in media to grow anaerobic species, which are typically very fastidious in their nutrient requirements • The growth of anaerobic microorganisms, and examination of their properties using in vitro and in vivo model systems, has now led us back to the understanding that different microorganisms have varying potential to cause disease.
Thus, the current concept of the processes involved in the development of periodontal diseases fall under the Specific Plaque Hypothesis (Loesche,1976 • The Specific Plaque Hypothesis states that disease results from the action of one or several specific pathogenic species and is often associated with a relative increase in the numbers of these organism found in plaque. • A form of Koch's Postulates specifically oriented to the situation in periodontal diseases has been proposed by a microbiologist by the name of Socransky (Socransky & Haffajee, 1992).
Socransky's criteria for periodontal pathogens are as follows: • ASSOCIATION: A pathogen should be found more frequently and in higher numbers in disease states than in healthy states • ELIMINATION: Elimination of the pathogen should be accompanied by elimination or remission of the disease. • HOST RESPONSE: There should be evidence of a host response to a specific pathogen which is causing tissue damage. • VIRULENCE FACTORS: Properties of a putative pathogen that may function to damage the host tissues should be demonstrated. • ANIMAL STUDIES: The ability of a putative pathogen to function in producing disease should be demonstrated in an animal model system.
The two periodontal pathogens that have most thoroughly fulfilled Socransky's criteria are Actinobacillus actinomycetemcomitans in the form of periodontal disease known as Localized Juvenile periodontitis (LJP), and Porphyromonas gingivalis in the form of periodontal disease known as adult periodontitis. • Selected properties of these microorganisms that have been associated with disease are summarized in the following tables.
Evidence implicating Actinobacillus actinomycetemcomitans as a periodontal pathogen(Adapted from Socransky, 1992) • CRITERION OBSERVATIONS • Association Elevated in lesions of Juvenile Periodontitis, and some lesions of Adult Periodontitis • Elevated in "active" Localized Juvenile Periodontitis (LJP) lesions • Detected in apical region of periodontal pocket or in tissues of LJP lesions • Unusual in health or gingivitis • Elimination Elimination associated with clinical resolution of disease • Species found in recurrent lesions • Host Response Elevated systemic and local antibody levels in Juvenile Periodontitis • Virulence Factors Leukotoxin, collagenase, endotoxin, epitheliotoxin, fibroblast inhibitory factor, bone resorption-inducing factor • Animal Studies Disease induced in gnotobiotic rats
Evidence implicating Porphyromonas gingivalis as a periodontal pathogen (Adapted from Socransky, 1992) CRITERION OBSERVATIONS • Association Microorganism is elevated in periodontitis lesions Unusual in health or gingivitis • Elimination Suppression or elimination results in clinical resolution • Species found in recurrent lesions • Host Response Elevated systemic and local antibody in periodontitis • Virulence Factors Collagenase, trypsin-like enzyme, fibrinolysin, immunoglobulin degrading enzymes, other proteases, phospholipase A, phosphatases, endotoxin, hydrogen sulfate, ammonia, fatty acids and other factors that compromise PMN function • Animal Studies Onset of disease correlated with colonization in monkey model • Key role in mixed infections in animal models
Other species that have been implicated as pathogens, including Fusobacterium nucleatum, Prevotella intermedia, Eikenella corrodens, Campylobacter rectus, Bacteroides forsythus, and the oral spirochetes of the genus Treponema. • It is important to note that the disease processes involve not only pathogenic microorganisms, but also a susceptible host. • Further, many microorganisms function to the benefit of the host, by inhibiting the growth of potential pathogenic species. One example of such an interaction is Streptococcus sanguis, which produces hydrogen peroxide that is lethal for Actinobacillus actinomycetemcomitans.
"Ecological Plaque Hypothesis" • The data from the mixed cultures studies described above, and from other work, provide an argument for plaque mediated diseases being viewed as a consequence of imbalances in the resident microflora resulting from an enrichment within the microbial community of these "oral pathogens.". • Potentially cariogenic bacteria may be found naturally in dental plaque, but these organisms are only weakly competitive at neutral pH, and are present as a small proportion of the total plaque community • In this situation, with a conventional diet, the levels of such potentially cariogenic bacteria are clinically insignificant,and the processes of de- and re-mineralization are in equilibrium.
If the frequency of fermentable carbohydrate intake increases, then plaque spends more time below the critical pH for enamel demineralization (approximately pH 5.5). The effect of this on the microbial ecology of plaque is two-fold. • Conditions of low pH favor the proliferation of acid-tolerating (and acidogenic) bacteria (especially mutans streptococci and lactobacilli), while tipping the balance towards demineralization. Greater numbers of bacteria such as mutans streptococci and lactobacilli in plaque would result in more acid being produced at even faster rates, thereby enhancing demineralization still further. • Other bacteria could also make acid under similar conditions, but at a slower rate. These bacteria could be responsible for some of the initial stages of demineralization or could cause lesions in the absence of other (more overt) cariogenic species in a more susceptible host. • If aciduric species were not present initially, then the repeated conditions of low pH coupled with the inhibition of competing organisms might increase the likelihood of successful colonization by mutans streptococcior lactobacilli.
Key features of this hypothesis are that • (a) the selection of "pathogenic" bacteria is directly coupled to changes in the environment and • (b) diseases need not have a specific etiology; any species with relevant traits can contribute to the disease process. • Thus, mutans streptococci are among the best adapted organisms to the cariogenic environment (high sugar/low pH), but such traits are not unique to these bacteria. Strains of other species, such as members of the S. mitis-group, also share some of these properties and therefore will contribute to enamel demineralization • A key element of the ecological plaque hypothesis is that disease can be prevented not only by targeting the putative pathogens directly, e.g. by antimicrobial or anti-adhesive strategies, but also by interfering with the selection pressures responsible for their enrichment
Strategies that are consistent with the prevention of disease via the principles of the ecological plaque hypothesis include the following: • (a) Inhibition of plaque acid production, e.g. by fluoride containing products or other metabolic inhibitors. Fluoride not only improves enamel chemistry but also inhibits several key enzymes, especially those involved in glycolysis and in maintaining intracellular pH. Fluoride can reduce the pH fall following sugar metabolism in plaque biofilms,prevent the establishment of conditions that favor growth of acid-tolerating cariogenic species. • (b) avoidance between main meals of foods and drinks containing fermentable sugars and/or the consumption of foods/drinks that contain non-fermentable sugar substitutes such as aspartame or polyols, thereby reducing repeated conditions of low pH in plaque. • (c) the stimulation of saliva flow after main meals, e.g. by sugar-free gum. Saliva will introduce components of the host response, increase buffering capacity, remove fermentable substrates, promote re-mineralization, and more quickly return the pH of plaque to resting levels.
Benefits of dental plaque • They play a critical role in the normal development of physiology of the host. Germ free animals have altered mucosal surfaces, poor nutrient absorption, suffer from nutritional deficiencies and have impaired host defenses. • In mineralization of early carious lesions (white spot) • Resident microflora also reduces the risk of infection by acting as a barrier to colonization by exogenous species termed colonization resistance. Reduction of colonization resistance can result in overgrowth of minor components of microflora, establishment of exogenous species which can lead to pathological changes.
Plaque in children • In Children as in adults the cause of gingivitis is plaque, local conditions and poor oral hygiene favor its accumulation • In preschool children the gingival response to bacterial plaque has been found to be markedly less than that in adults. • Dental plaque appears to form more rapidly in children age 8 to 12 years than in adults • Calculus is uncommon in infants; it occurs approx 9%of children 4 to 6 years of age • In 18 % of those 7 to 9 years and in 33% to 43% of those 10 to 15 years
Plaque as a biofilm • Biofilm is a well-organized ,co-operating community of microorganisms. they form under fluid conditions. • bacteria in the biofilms produce compounds that the same bacteria do not produce in cultures. also the matrix surrounding the colonies acts as a protective barrier. • substances produced by bacteria within the biofilm are retained and concentrated which fosters metabolic interactions among the different bacteria
Properties of a biofilm • cooperating community of various types of microorganisms • microrganisms are arranged in microcolonies • microrganisms are surrounded by protective matrix • within the micromolecules are differing environment • microrganisms have a primitive communication system • microrganisms in biofilms are resistant to antibiotics, antimicrobials and host response.
Significance of plaque as a biofilm • Some bacteria alter their pattern of gene expression when cells encounter a surface. Attached cells up-regulate genes associated with expolymer synthesis and can modify upto30% of surface proteins • Increased resistance of biofilms to antimicrobial agents upto 2-1000 fold. • The surface of a biofilm may restrict the penetration of an antimicrobial agent; some charged inhibitors can bind to oppositely charged polymers that make up the biofilm matrix • Environment in the depth may be unfavorable for optimal action of certain drugs • A susceptible pathogen may be rendered resistant if neighboring cells produce a neutralizing or drug degrading enzyme. • In addition biofilms provide an ideal environment for transfer of resistance genes.
CONCLUSION • Despite tremendous increases in our understanding of the pathogenic properties of specific plaque microorganisms and the role of specific microorganisms in the disease process, current therapy in periodontics is largely non-specific. • The treatments that we utilize (e.g., oral hygiene measures, debridement by scaling and root planning, or even the currently available mouthwashes) are oriented towards reducing the accumulation of plaque on the teeth. • Future developments in periodontics will involve the development of therapies which prevent the colonization or growth of specific microorganisms that are known to function as pathogens in this environment.