Download
1 / 4
40 likes | 340 Views
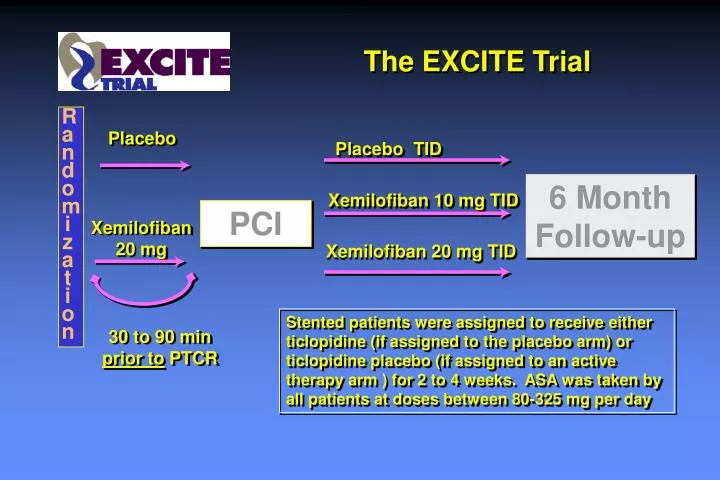
The EXCITE Trial. Randomization. Placebo. Placebo TID. 6 Month Follow-up. Xemilofiban 10 mg TID. PCI. Xemilofiban 20 mg. Xemilofiban 20 mg TID.

E N D
The EXCITE Trial Randomization Placebo Placebo TID 6 Month Follow-up Xemilofiban 10 mg TID PCI Xemilofiban 20 mg Xemilofiban 20 mg TID Stented patients were assigned to receive either ticlopidine (if assigned to the placebo arm) or ticlopidine placebo (if assigned to an active therapy arm ) for 2 to 4 weeks. ASA was taken by all patients at doses between 80-325 mg per day 30 to 90 min prior to PTCR
0.20 Treatment Placebo Xemilofiban 10 mg Xemilofiban 20 mg 0.15 Cumulative Event Rate 0.10 0.05 0 0 1 2 3 4 5 6 7 Month from Randomization Primary Efficacy Analysis(Death, MI, and Urgent Revascularization)
Comparison Among Oral Agents 2nd Generation 1st Generation Oral IIb/IIIa inhibitors RoxifibanOrbofibanSibrafibanXemilofiban TrialRocket OPUS-TIMI16 Symphony EXCITE IIb/IIIa selective +++ +++ +++ +++ Binding TightlyCompetitive Competitive Competitive bound “Off rate” 7 mins seconds seconds seconds Peak of Onset 3-6h 4-6h 4-6h 2-3h Half-life 24 h 8-10h 11h 4-5h Excretion Plt. Dissoc. Renal Renal Renal Dosing QD BID BID TID Low Peak/trough +++ ++ ++ + Intra-pt variability + ++ ++ ++ Inter-pt variability ++ ++ ++ ++ Plts < 50,000 <0.5% 0.6% <0.5% 0.5% Plts Pro-aggreg. No Yes - Yes CP Cannon 2000
Oral Antiplatelet Therapy in the New Millennium • Future Directions - Oral IIb/IIIa inhibitors: 1. Need to optimize dosing • Mimic stable effect of IV drugs • Reduce inter- and intra-patient variability • ? Use bedside platelet test to adjust dose 2. Test “second generation” drugs (tight IIb/IIIa binding) • ASA and ADP antagonists • Proven benefit in large trials • Both decrease platelet activation • Combination ASA/Clopidogrel being tested CP Cannon 2000