Download
1 / 32
350 likes | 506 Views
Explore the history, pathogenesis, and treatment of textile dust-related lung diseases like byssinosis. Learn about the clinical features, diagnosis, and prevention strategies. Discover the impact of occupational hazards in the textile industry over the past 300 years.

E N D
Byssinosis & Other Textile Dust related Lung diseases By: Firoozeh M,M.D
History Work in textile industry , as an occupational hazard from 300 years ago. Peculiar form of asthma among card Flax & hemp workers (Ramazzini 18th century). Cotton dust standards & medical surveillance in the 1970 in United states. Increasing prevalence rates in the developing countries.
Although Natural fibers are common limited numbers can be used for textile: 1-Physical properties Length Strength Pliability Elasticity 2- Difficulty in physically separating cellulose fibers from other vegetable components.
Early phases of the process are dustier ( Opening, Picking, Carding) Dissemination of respirable fine dusts in grounding by mechanical separator
Pathogenesis Etiologic agents and pathogenesis Remain unclear. The most common hypotheses: The release of mediators. Immunologic mechanisms. Airway reactions to specific dust components.
Release of mediators Cross shift changes in exposure: Release of both performed & de novo synthesized mediators. Elevated levels of histamine in cotton workers Higher levels on the first day of re-exposure & related to level of dust exposure Lower blood levels of histamine in continuouse exposure Histamine associated with only a short time airway response No consistent block of reactions with antihistamines but mast cell stabilizers blunt the response.
Immunologic mechanisms Immediate hypersensitivity Immune complex formation Complement activation Long period of time before onset of symptoms(indicate sensitization) Slow progressive damage Delay onset of symptoms
specific cotton dust components At least 50 biologically active components Endotoxin -A good index of acute bronchoconstrictor esponse - Not the principal bronchoconstricting agent Tannins -PMN recruitment - Plt aggregation , mediator release - Toxic effect on respiratory epithelial & endothelial cells - Inhibits chloride secretion of airway epithelium - Desensitizing tracheal epithelial cells to β agonists - Don’t produce direct airway construction
Clinical features 1- Work related respiratory complaints (Monday symptoms) 2- Changes in pulmonary function After working a number of years,worker describes chest tightness beginning on the first day of work week afternoons. The tightness subsides that evening , worker is well in reminder of week , and re-experience symptoms on the first day of following work weeks. Symptoms may continue unchanged or progress
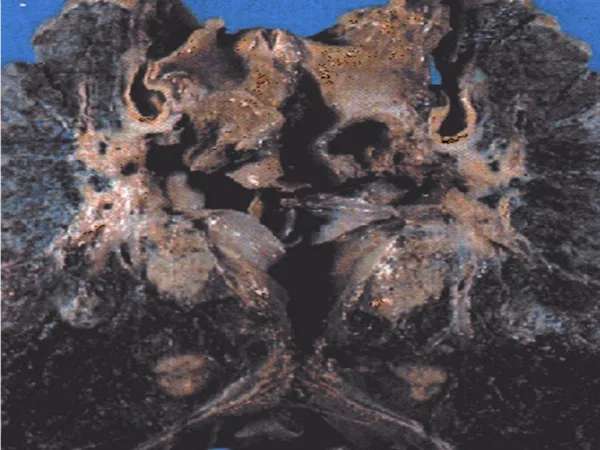
Clinical features At chronic phase : - Exertional dyspnea - Non productive cough Across shift decrease in lung function,which maybe present on other work days even in absence of symptoms.
Grading 0 : NL,No symptoms of chest tightness or cough. ½ : Occasional chest tightness or cough or both on 1th day of working week. 1 : chest tightness on every 1th day of working week. 2 : chest tightness on every 1th day & other days of the working week. 3 : Grade 2 symptoms + permanent ventilatory incapacity.
In addition to classic byssinosis ,other symptoms: Mill fever : Fever,cough,chill,rhinitis at first contact with mill or return after prolong absence . chest tightness(-) Weaver’s cough: Asthmatic condition with fever in new & senior workers,persist for months. Mattress makers’ fever: Acute outbreak of fever & constitutional symptoms,in using low grade cotton. Chronic bronchitis
Mortality Signficant mortality from non malignant respiratory diseases, specially chronic lung diseases. Low mortality rates from lung cancer .
Diagnosis History Physical examination Lung function Lab evaluation Challenge testing Immunologic testig Across shift Reduction in change in FEV1FEV1 F0 None(<5%) None(>80%) F1/2 Slight(6-12%) None F1 Definite(>20%) None F2 Slight/moderate (60-75%) F3 Moderate/Severe (<60%)
Treatment Bronchodilating agents Antihistamines Disodium cromoglycate Aerosolized Steroids
Prevention Dust abatement Medical surveillance with transfer policies for affected workers Treatment of raw cotton to eliminate toxic factors Smoking cessation
OSHA standards Medical surveillance - PFT annually - If baseline Lung function is < 80% predicted or decrease of FEV1> 5-10% over work shift PFT semiannually. - If Lung function is < 60% predicted refer to complete examination.
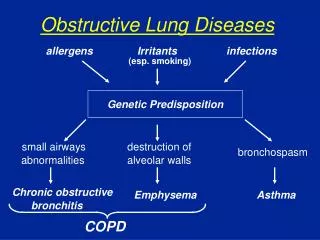
Definition: Presence of cough with phlegm at least 3 months, for at least 2 years. Progressive Airflow limitation that is not fully reversible. Abnormal inflamatory response of lung to noxious particles or gases. Morbidity Prevalence :4% in united states
Risk factors: - Tobacco smoke - Occupational dust & chemicals - Indoor/Outdoor air pollution Occupational COPD: Chronic bronchitis in a patient with hx of chronic exposure to pro-inflammatory agents in workplace air.
Epidemiology Ranked as the 4th leading cause of death. Ranked as 12th leading cause of disability. Increase with age. Equal prevalence among men & women. The rate increasing faster among women. Occupational exposures:15% of burden of COPD.
Occupational risk factors Chronic or repeated exposure to: Organic particulate matter Bioaerosols Combustion products Mineral/metal particulate matter or fume Irritant gases & vapours
Mineral particulate & fibers Mining ,tunnelling,building & road construction,cement work,stone carving,farming,… Prevalence rate of COPD in non-smoker miners:20% in smoker miners: 60% Silica exposure: Higher COPD retes , mortality from bronchitis, emphysema & asthma Asbestos & Carbon black exposure: airflow obstruction & COPD
Metal fumes,Irritant gases,Combustion products Mining,smelter workers,rubber manufacturing, welders, fire fighters,… Risk higher among atopic workers
Organic dusts Textiles, agricultur, baking ,wood & paper industries. Exposure to Allergenic & non allergenic organic dusts: Asthma HP COPD & chronic bronchitis
Agriculture Inflammatory process in the airway from: Dusts : grains,animal feed,soils Gases & Fumes: manure gases & disinfectants Micro-organisms: endotoxin & fungal components Chronic airway disease
Environmental tobacco smoke in workplace In non smoker emploees in high ETS exposure : Airflow obstruction Hair levels of nicotine
Assessment of exposure Detailed occupational history (specially for dusts,gases,fume exposure) Ask about the year of beginning & ending the job(duration). How often exposed todusts,gases,fume ?(intensity)
Management For the patient still exposed to hazards: recommendation should be made to reduce or eliminate the exposure. For the patient no longer exposed to hazards: the disease should be labelled as potentially occupational.
Prevention Rapid decline in FEV1(but still in the NL range) in young exposed workers worse prognosis. Patient should be made aware of his /her decline in Pulmonary function . Increase recognition & reporting of disease. Willingness of employers to act to reduce exposure to hazards.