Download

1 / 40
420 likes | 578 Views
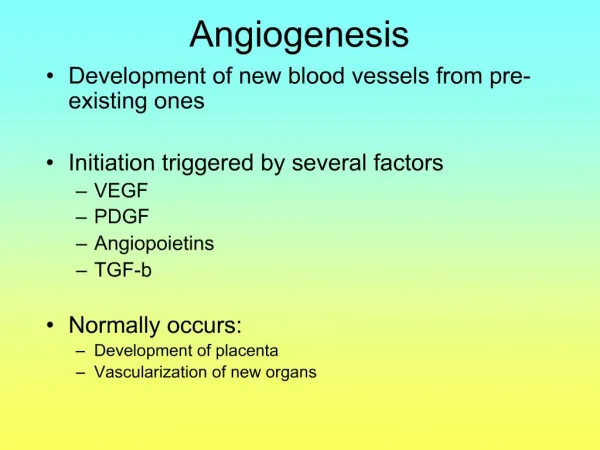
Meta-analyses confirm survival benefit with chemotherapy 1990s. Tumour growth is angiogenesis dependent Judah Folkman 1971. Routine identification of EGFR mut+ve & TKIs therapy 2010-11. Discovery of cisplatin 1965. Discovery of paclitaxel 1967. VEGF gene identified

E N D
Meta-analyses confirmsurvival benefit withchemotherapy 1990s Tumour growth is angiogenesis dependent Judah Folkman 1971 Routine identification of EGFR mut+ve & TKIs therapy 2010-11 Discoveryof cisplatin 1965 Discoveryof paclitaxel 1967 VEGF gene identified and EGFR isolated 1980s Bevacizumab / TKIsimprove survival in mol.unselected NSCLC 2000s
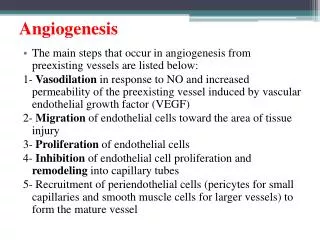
Dimerisation of ligand-bound receptors • ATP binding and phosphorylation of tyrosine-kinase domain TKI TKI EGFR TKI blocks ATP binding and prevents activation of TK domain • Activation of two major intracellular signalling pathways • Cellular response to signals Ciardiello F and Tortora G. , NEJM 2008
GEFITINIB/ERLOTINIB CLINICAL DEVELOPMENT INTACT 1&2 Giaccone, JCO 2004 Herbst, JCO 2004 NEJ 002 Maemondo, NEJM 2010 INTERESTKim, Lancet 2008 IPASS Mok, NEJM 2009 GEFITINIB ISEL Thatcher, Lancet 2005 WJTOG 3405 Mitsudomi, Lancet 2010 IDEAL 1&2 Fukuoka, JCO 2003 Kris, JAMA 2003 INVITE Crinò, JCO 2008 FIRST-SIGNAL Han, JCO 2012 2000 2003 2004 2005 2007 2008 2009 2010 2011 2012 OPTIMAL Zhou, Lancet Oncol 2011 TALENTGatzmeier, JCO 2007 TRIBUTEHerbst, JCO 2005 SATURN Cappuzzo, Lancet Oncol 2010 ERLOTINIB EURTAC Rosell, Lancet Oncol 2012 TRUST Reck, JTO 2010 BR 21 Shepherd, NEJM 2005 Phase I-II Perez-Soler, JCO 2004 Molecular target Clinical/Histological selection Unselected population
Europe SLCG, 2009 FIELT, 2011 EURTAC, 2012 Asia IPASS,2009 OPTIMAL, 2011 First-SIGNAL, 2012 USA Japan WJTG, 2010 Sequist, 2008 CALGB, 2011 NEJSG, 2010
IRESSA PAN ASIA STUDY DESIGN Endpoints • Primary • PFS (non-inferiority) • Secondary • Objective response rate • Quality of life • Disease related symptoms • Overall survival • Safety and tolerability • Exploratory • Biomarkers • EGFR mutation • EGFR gene copy number • EGFR protein expression • Patients • Age ≥18 years • Life expectancy≥ 12 weeks • Adenocarcinoma histology • Never smokers or light ex-smokers* • PS 0-2 • Stage IIIB/IV • Measurable disease Gefitinib250 mg/day 1:1 randomization Carboplatin AUC 5/6 Paclitaxel 200mg/m2 3 wkly *Never smokers:<100 cigarettes in lifetime; light ex-smokers: stopped 15 years ago and smoked 10 pack yrs Carboplatin/paclitaxel was offered to gefitinib patients upon progression T Moket al, NEJM 2009
EGFR mutation by PCR sequencing 437 samples (36%) 261 positive (60%) T Moket al, NEJM 2009
Gefitinib Carbo / pac p=0.0001 9.5 ms 6.3 ms T Moket al, NEJM 2009
Gefitinib Carboplatin / paclitaxel S Thongprasertet al, JTO 2011
PD R PD Gefitinib 250 mg/day P.O. daily, • Patients • Chemo-naïve • Age 18-75 years • Adenocarcinoma • Never smoker • ECOG PS 0-2 • Stage IIIB or IV 1 Female vs. Male PS 0, 1 vs. 2 Stage IIIb vs. IV PrimaryEndpoint: OS 1 Gemcitabine 1250 mg/m2 (D1 & D8)Cisplatin80 mg/m2 (D1) q 3 weeks x 9 cycles * Gemcitabine+Cisplatin Dose: Same as in INTACT-1 and TALENT J-Y Han et al, JCO 2012
9.2 ms HR=0.49, p <.001 6.3 ms T Mitsudomi et al, Lancet 2009
HR= 0.30 (0.22-0.41) p value <.001 10.8 ms 5.4 ms M Maemondoet al, NEJM 2010
1. P Jänne et al, WCLC 2011/2. R Rosellet al, NEJM 2009/ 3. J De Grève et al, ASCO 2011
73.0* * * MeasurableDisease T Mok, PeerVoice 2011 (modified)
1.Mok et al, NEJM 2009; 2.Zhou et al. Lancet Oncol 2011; 3.Rosell et al, Lancet Oncol 2012; * TKI arm ** MeasurableDisease
*For IPASS, First-SIGNAL and CALGB30406 these data are for all patients in TKI arm (not limited to EGFR MUT+ group)ALT = alanineaminotransferase; AST = aspartateaminotransferase 1Zhou, et al. Lancet Oncol 2011; 2Rosell, et al. NEJM 2009; 3Janne, et al. ASCO 2010; 4Mok, et al. NEJM 2009 5Lee, et al. WCLC 2009; 6Mitsudomi, et al. Lancet Oncol 2010; 7Maemondo, et al. NEJM 2010; 8 Rosell, Lancet Oncol 2012
TK-Is AND DIFFERENT EXPOSURE Standard dosing ~MTD MTD Cmax = maximum plasma concentrationAUC = area under the curve 1Hidalgo M, et al. J ClinOncol 2001;19:3267–792Ranson M, et al. J ClinOncol 2002;20:2240–50