Download
1 / 22
230 likes | 507 Views
Free fetal DNA. Sarah Whelton West Midlands Regional Genetics Laboratory. Summary. Fetal material – origin and kinetics in maternal plasma Where are we with now with non invasive prenatal diagnosis? Birmingham testing strategy for fetal sex determination Improvements on current practice

E N D
Free fetal DNA Sarah Whelton West Midlands Regional Genetics Laboratory
Summary • Fetal material – origin and kinetics in maternal plasma • Where are we with now with non invasive prenatal diagnosis? • Birmingham testing strategy for fetal sex determination • Improvements on current practice • Future developments for aneuploidy testing
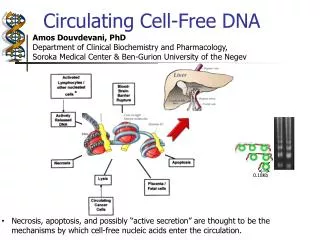
Fetal material: Origin and kinetics Intact fetal cells in maternal circulation erythroblasts trophoblastic cells leucocytes Problems: Occurrence is rare and requires complex enrichment and identification 1-6 fetal cells per millilitre of maternal blood Studies show a low sensitivity rate for fetal sex determination (95%) and a false-positive rate was 11.1% (Bianchi et al, 2002) Persist for years after pregnancy
Fetal material: Origin and kinetics Cell free fetal DNA • Originates from trophoblast • Detectable from 5 weeks’ and increases with gestation • 3 – 6% of total circulating cell free DNA • Exist in small fragments of around 300bp of which 80% are less than 200bp • Cleared from circulation within 30 minutes of delivery
Using ffDNA for non-invasive prenatal testing • Sexing– already carried out • RhD status – already carried out • Single gene disorders –few have been reported • Aneuploidy detection – long term aim
Fetal Sexing Testing sex for • X-linked disorders such as DMD and Fragile X –avoid unnecessary invasive procedures • CAH – avoid treatment of dexamethasone Sample requirements • Fresh maternal blood • Received within 24h • ~10mls for a min of 4mls plasma • Dealt with efficiently to avoid cell lysis • Introduction of Streck tubes for stabilisation of maternal cells
DNA extraction • 2 extraction methods: • EZ1 Qiagen DSP Virus: 800ul plasma • Uses magnetic bead particle technology • Automated • 40 min • Qiagen QIAamp mini spin kit: 1ml plasma • Silica gel membrane to bind DNA • Labour intensive • 30-40 min • Both kits contain carrier RNA which is integral to the binding of small fragmented molecules
Real-Time PCR for fetal sexing • Real time PCR or quantitative PCR (qPCR) measures the amount of PCR product throughout the course of the reaction. • Highly sensitive • Only target sequences present in the sample are amplified • Offer a closed system for analysis with minimal errors How does it work? Taqman chemistry: Set of primers covering your gene of interest and a hydrolysis probe specific to the template sequence. This probe contains 2 distinct features. • A reporter dye such as FAM, VIC (ABI platforms) and JOE, HEX and Cy5 on other platforms. • The quencher which acts to suppress the fluorescence of the reporter dye when in close proximity. When the reporter and the quencher are in close proximity then there is no fluorescence. Examples: Dyes such as TAMRA or non fluorescent quenchers MGB (ABI), Black Hole Quencher (BHQ)
Real-Time PCR for fetal sexing • Binging of probe and primers to target sequence • Polymerisation of the forward strand • The 5 prime nuclease activity of the Taq starts to displace the nucleotides of the probe. • Cleavage of the reporter dye increases the distance of the reporter to the quencher and they are no longer in close proximity • Release of fluorescence • The taq finishes synthesis of the target strand so it can then be used in the next round of PCR.
Real-Time PCR for fetal sexing • Binging of probe and primers to target sequence • Polymerisation of the forward strand • The 5 prime nuclease activity of the Taq starts to displace the nucleotides of the probe. • Cleavage of the reporter dye increases the distance of the reporter to the quencher and they are no longer in close proximity • Release of fluorescence • The taq finishes synthesis of the target strand so it can then be used in the next round of PCR.
Birmingham: Fetal sexing Run two extractions (EZ1 and QIAamp) on each sample SRY – fetal sex assay (8 replicates) CCR5 – universal marker for control of DNA extraction (2 replicates) Standard curves for SRY and CCR5 for quantification. A female is inferred from a negative SRY reaction but the amplification of CCR5 suggests the extraction has worked A male result showing amplification in the SRY assay alongside the CCR5 amplification.
Improvements on current practice Females are inferred from the absence of SRY signal but there is a risk that a sample with low fetal DNA may not amplifying enough signal to be detected. Eg. Extraction errors or just low amounts of fetal DNA in the sample (low gestation). The search for an independent fetal marker Y Chromosome: only applicable to 50% of pregnancies Polymorphic markers: (Finning and Chitty, 2008)panel of bi-allelic polymorphic markersfrom the plasma DNA and maternal DNA using RQ-PCR. Problems: uninformative in 60% of samples and expensive Methylation: Differences in maternal and fetal status of certain promoter regions. E.g. MAPSIN and RASSF1A
RASSF1A The promoter is differentially methylated in placenta relative to maternal cells. • hypermethylated in the placenta and hypomethylated in maternal blood cells. • This pattern of methylation difference allows methylation sensitive restriction enzymes to remove the maternal unmethylayed copies of RASSF1A, leaving behind fetal RASSF1A, which can then be detected by downstream assays such as real time PCR.
RASSF1A development Detection of RASSF1A signal denotes the presence of fetal material. IMPORTANT: to ensure that the restriction enzyme digest has gone to completion, as any undigested maternal sequence will look like fetal DNA Controls B-actin is unmethlyated in both maternal and fetal material. When run in parallel should be completely negative if the restriction enzyme digest has worked. Undigested RASSF1A and b-actin: to ensure that it is the restriction enzyme digest which is causing this to be negative. DNA extracted form 1ml Plasma using the Qiamp DSP Virus Kit Hha1 BstU1 37ºC for 60 min Methlyation sensitive Digest Mix No Restriction enzyme mix SRY mix Real-time PCR RASSF1A P P Beta-actin x P SRY P/x
RASSF1A development SRY RASSF1A Late RASSF1A signal Range: 38-41 Cts compared to 35-38 for SRY Due to PCR inhibition from Restriction enzyme buffer. RASSF1A - undigested Bata-actin - undigested
Future developments for aneuploidy testing RAPID - Reliable Accurate Prenatal non-invasive Diagnosis plans to evaluate the methods available for non invasive prenatal testing. • Helen White (Wessex) currently evaluating methods available for the detection of Downs Syndrome (May 2010) • Quantitative SNP analysis from ffRNA • Digital PCR • Massively parallel sequencing of cfDNA • RAPD: Plans to develop NIPD for aneuploidy
Massively Parallel genomic sequencing of cell free DNA • Previous groups have demonstrated the use of: RNA-SNP allelic ratio approach Relative chromsome dosage by digital PCR • Limited as they are locus specific Chiu et al 2008 proposed a method independent of gene locus to quantify the amount of Chr21 sequences in maternal plasma. • Potentially every DNA fragment originating from an aneuploid chromosome could contribute to the measurement of that Chr in maternal plasma. • There are more quantifiable sequences than the number of DNA molecules that could act as templates for detection by gene locus specific assays.
Fetal DNA (red) in a background of maternal DNA (black). A representation of the sample is taken. One end of each plasma DNA molecule is sequenced for 36bp using Solexa Sequencing by synthesis approach. Origin of each 36bp is mapped to the Human reference genome Calculation of % of chr of interest and the z score compared with reference sequence
Chiu et al 2008 • 28 Maternal samples • 14 T21 • 14 Nornal
Summary • Shows a proof of principle for the detection of aneuploidy • As the approach is locus independent it can be used for all pregnancies • More work needs to be done and on a larger scale The main disadvantages of this technique is that it is currently very expensive and requires a large amount of interpretation - With advances in technology this could be addressed and could incorporate high throughput analysis.
Dennis Lo predicts… By 2020… “the sequencing of the whole fetal genome from maternal plasma would already have been achieved” “the main technology for NIPD would be that based on single molecule analysis methods. Digital PCR and Massively parallel DNA sequencing” “a large number of large scale clinical trials testing the diagnostic accuracy of this technology would have been published” “the sequencing and data analysis steps to be completed within half a working day”