Download
1 / 49
690 likes | 1.21k Views
Spinal Vascular Malformations. Sohail Bajammal February 2, 2009. Acknowledgement. Dr. Aleksa Cenic. Outline. Embryology Anatomy Classification Clinical presentation Treatment. Embryology of the Spinal Vascular Network. 4 stages Congenital theory of AVMs:

E N D
Spinal Vascular Malformations Sohail Bajammal February 2, 2009
Acknowledgement Dr. Aleksa Cenic
Outline • Embryology • Anatomy • Classification • Clinical presentation • Treatment
Embryology ofthe Spinal Vascular Network • 4 stages • Congenital theory of AVMs: • 20% of patients with intradural AVMs have other associated congenital vascular malformations: intracranial AVMs, cerebral aneurysm, vascular agenesis, hemangioblastoma, Rendu-Osler-Weber syndrome, Klippel-Trenaunay-Weber syndrome • Present in younger patients • Distributed throughout the entire spinal axis
Stage I “Primitive Segmental Stage” • Week 2-3 gestation • 31 pairs of segmental vessels originate from paired dorsal aortas grow toward the neural tube along the developing nerve roots • Segmental vessels divide into ventral & dorsal branches and form capillary networks on the ventrolateral surface of the neural tube • These networks develop into paired primitive ventral arterial tracts, the precursors of the anterior spinal artery
Stage II “Initial Stage” • Week 3-6 gestation • Development of the dorsal arterial anastomosis • Longitudinal venous channels develop on both ventral and dorsal spinal cord surfaces • These channels expand and give rise to interconnected capillary network • AVM theoretically happens during this stage
Stage III “Transitional Stage” • 6th week – 4th month gestation • Formation of the adult pattern of vascular supply • The primitive ventral longitudinal arterial tracts fuse and the number of segmental arteries is reduced • By 10 weeks, adult patterns are present
Stage IV “Terminal Stage” • After 4th month • Maturation and increased tortuosity of the major spinal cord vessels
Arterial Anatomy • Anterior spinal artery: • arises from the fusion of a contribution from each of the vertebral arteries • supplies the ventral 2/3 of the cord • narrows as it descends but reinforced by blood vessels at some segmental levels • Paired posterior spinal arteries: • run the length of the spine • supply the posterior 1/3 of the cord
Arterial Anatomy • At each segmental level: a dorsal ramus of the segmental artery enters the intervertebral foramen and gives rise to 3 branches: • Dural branch: to dura • Radicular branch: to nerve root • Medullary branch: • Augments the flow to the anterior spinal artery • During the 3rd stage of fetal development, most of the medullary branches involute distal portion of the cord relatively ischemic • Somewhere between T8 & L2, especially on the left: the medullary branch does not involute and becomes the artery of Adamkiewicz
Venous Anatomy • Coronal venous plexus: • A plexus on the cord surface • Formed by coalescence and anastomosis of radial veins • Epidural venous plexus: • At segmental levels, medullary veins leave the coronal plexus and exit the intervertebral foramen to join the epidural plexus • The plexus communicates with the venous sinuses of the cranial dura • It drains into the ascending lumbar veins and the azygous venous system
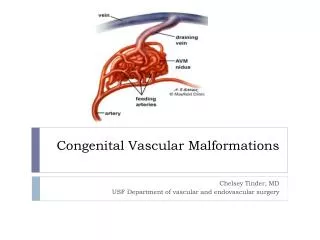
Spinal Vascular MalformationsTerminology • Definition: abnormalities of the arteries or veins surrounding the spinal column, spinal cord, and nerve roots • AV fistula (AVF): direct communication between artery & vein • AV malformations (AVMs): multiple complex communications • Nidus: the core of an AVM that appears angiographically and anatomically as a conglomeration of vessels because of the superimposition of arteries and veins.
Spetzler et al. Modified classification of spinal cord vascular lesions. J Neurosurg (Spine 2) 2002.
Incidence • Rare cause of neurologic dysfunction • 5% of all intraspinal pathology • Occur throughout the spine • Affect any age group, majority: 30-50 • Better diagnosis and management with improved techniques of spinal angiography, MRI, MRA and endovascular surgery O`Toole and McCormick. Chapter 83: Vascular Malformations of the Spinal Cord. Rothman-Simeone The Spine. 5th Edition
Clinical Presentation • Haemorrhage • Myelopathy • Radiculopathy • Back pain
Pathophysiology of Symptoms • Depends on the type of the AVM • High-flow: • Ischemia • Hemorrhage • Slow-flow: • Venous congestion • Mechanical compression of the spinal cord and roots
Classification • Many exist • Most common: 4 types based on the location and angioarchitecture • Anatomical: intradural vs extradural • Presence or absence of AV shunts • Recent: Spetzler 2002
4 Types • Type I: Dural AV Fistula • Type II: Glomus AVMs • Type III: Juvenile AVMs • Type IV: Intradural AV Fistula
Type I (Dural AV Fistula) • The most common type • 60% of spinal AVF/AVM • Single AV connection within the dura of the nerve root sheath • Results in dilated arterialized coronal venous plexus
Pathophysiology of Type 1 • Slow-flow Intradural venous hypertension progressive spinal cord ischemia • Exercise (elevated intraspinal venous pressure) reversible ischemic symptoms • Venous hypertension may be exacerbated by structural changes in the veins • Venous thrombosis acute exacerbation
Clinical Presentation Type 1 • Mean age: 50yr • Men 4 times more common • Majority: thoracic and thoracolumbar • Symptoms: insidious back and leg pain, mild sensorimotor dysfunction (like spinal stenosis) • Signs: mixed UMNL and LMNL and patchy sensory loss.
Natural History of Type 1 • Inevitable progression of symptoms • Episodes of acute worsening • e.g., Foix-Alajouanine syndrome • If untreated: wheelchair dependence within 6mo to 3 years after symptom onset • Preoperative neurologic status is the most important predictor of post-treatment outcomes. • Median time from symptom onset to diagnosis: 15 to 23 months.
Type II (Glomus AVMs) • Analogous to intracranial AVMs • Tightly packed nidus of dysmorphic arteries and veins in direct communication w/o capillary bed; over a short segment of the spinal cord • The nidus may be completely or partially intramedullary • Usually at the cervicothoracic junction
Pathophysiology of Type II • Vascular steal mechanism: High-flow lesion; AVM nidus acts as a low-resistance sump siphoning blood away from the surrounding normal spinal cord • Dysmorphic vessels susceptible to hemorrhage • Mass effect: myelopathy or radiculopathy
Clinical Presentation of Type II • Childhood or adult years • Acute presentation from subarachnoid or intramedullary hemorrhage is most common • Acute onset of severe neck or back pain “coup de poignard” approximates the level of AVM: typically the first symptom of AVM hemorrhage
Type III (Juvenile AVMs) • Arise in single or multiple adjacent somites thus intradural and extradural, may involve soft tissue and bone in addition to the cord • Diffuse shunts with normal spinal cord existing between loops of abnormal vessels • No distinct nidus • Metameric: tissue derived from the entire somite
Type IV (Intradural AVF) • Direct connection between an intradural artery and vein in the subarachnoid space without a definable nidus • Usually ventral, involves the anterior spinal artery • Sub classified: small, medium, large
Pathophysiology of Type III & IV • High-flow lesions • Vascular steal/ischemia • Hemorrhage • Mass effect
Type V • Type III lesions outside the spinal cord and dural (i.e., not truly metameric)
Diagnosis • MRI and MR angiography (MRA): useful for the initial screening of AVMs. Permit more targeted selective angiography • Selective spinal angiography: gold standard for definitive diagnosis and characterization
Treatment • Goal: total obliteration or excision of the abnormal shunt • If only partially reduce the shunt or address proximal feeders only recurrence
General Considerations of Surgical Treatment • Majority of AVMs are dorsal or dorsolateral standard posterior laminectomy of appropriate number of levels • Neuromonitoring: SSEPs & MEPs • Wide laminectomy • Dural opening with preservation of arachnoid
General Considerations of Endovascular Treatment • Continues to evolve • Advances in catheter technology, image resolution and embolization materials • Neuromonitoring and pharmacologic intra-arterial provocative testing (amobarbital and lidocaine) • Either primary or adjunctive role depending on the type of AVMs & expertise • Procedure of choice for type III • Type I & IV: attempts of embolization, if failed surgery. Some authors prefer surgery as first line • Type II: surgery remains the gold standard
Treatment of Type 1 • Historically, stripping of the long dorsal vein poor outcomes b/c removal of normal cord venous drainage • Now, excision of the dural fistula • Two-level hemilaminectomy and partial medial facetectomy to expose the dural root sleeve and foramen • Paramedian longitudinal dural incision: exposes the intradural nerve root and initial segment of draining vein • Several mm of the feeding radicular artery and intradural draining vein, cauterized, divided and excised along with a small window of dura on the root sleeve.
Outcomes of Type 1 Treatment • Neurologic improvement or stabilization in 70 to 99%. Motor and gait disturbances improve to a greater degree than sensory or sacral deficits • Surgery produces 98% fistula obliteration rate, endovascular embolization produces 25 to 66% obliteration rate. O`Toole and McCormick. Chapter 83: Vascular Malformations of the Spinal Cord. Rothman-Simeone The Spine. 5th Edition
Treatment of Type II • Preoperative endovascular embolization to shrink the size • Surgical excision: • Interruption of the feeding arteries first • If mainly intramedullary, midline myelotomy
Treatment of Type III • The most difficult to treat • They penetrate the spinal cord • Do not have well-defined margins (intramedullary, intradural-extramedullary, extradural) over many spinal segments • Generally unresectable. Palliative treatment with endovascular embolization, and/or surgery
Treatment of Type IV • Depends on the size and complexity • Small: surgical ligation is definitive • Posterior (or posterolateral) or anterior approach • Usually needs spinal instrumentation • Medium and large: endovascular embolization preferred as primary treatment or preopeative adjunct
Credits • Images from: • Spetzler et al • O`Toole and McCormick • Oldfield