Download
1 / 23
270 likes | 848 Views
NEISSERIA GONORRHOEA. By G.R.JAHNAVI. INTRODUCTION. Venereal disease - GONORRHOEA Gram negative Aerobic Arranged in pairs N.gonorrhoea is never a part of normal flora GONORRHOEA ―›flow of seed By GALEN in 130 AD. HISTORY. Neisser-gonorrhoeal pus

E N D
NEISSERIA GONORRHOEA By G.R.JAHNAVI
INTRODUCTION • Venereal disease - GONORRHOEA • Gram negative • Aerobic • Arranged in pairs • N.gonorrhoea is never a part of normal flora • GONORRHOEA ―›flow of seed • By GALEN in 130 AD
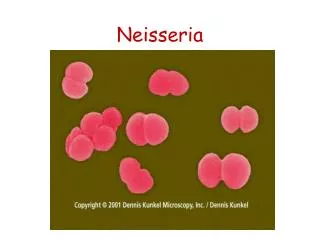
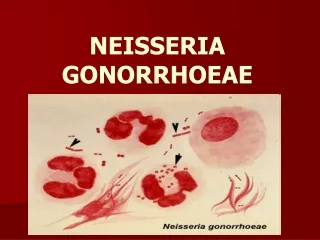
HISTORY • Neisser-gonorrhoeal pus • Bumm-cultured & proved pathogenecity MORHOLOGY • 0.6-1µm • Diplo cocci-kidney shaped • Pili - adhesion • inhibits phagocytosis • agglutinate RBC • Seen mostly in polymorphs
culture • Aerobic 5-10% CO2 • 35-36 °C • pH 7.2-7.6 • Fastidious .choclate agar .MHA • Selective medium-Theyer Martin Medium • (Vancomycin, Nystatin,Colistin)
Colony morphology • Small,round,transluscent, convex/umbonate,fine granular surface & lobate margins • Four types—T1,T2,T3,T4 • T1&T2—Piliated, autoagglutinable,virulent • Small ,brown colonies—p+&p++ • T3&T4 –nonpiliated & avirulent • Large, nonpigmented, granular colonies forming smooth suspensions ―› p- • Fresh isolates –T1 &T2 • Subcultures –T3&T4
BIOCHEMICAL REACTIONS • Catalase &*Oxidase ―› positive • Indole ―› negative • H2S ―› negative • Nitrate ―› negative • Only Glucose is utilised & acid formation is weak but no gas formation • *maltose not utilised
ANTIGENIC STRUCTURES • Pili • Trilaminar outer membrane protiens l, ll, lll. • Outer membrane―›LPS
pili―› .constant &variable regions .subunits pilins . antigenic & phase variations . attachment to host cells & inhibits phagocytosis
Protien l • Antigenic diversity • Antigenically Constant for a single strain • Two varients―›lA &lB • Serovars using monoclonal Ab’s • A ―›1-24 • B ―›1-32 • Protiens l & lll • Attacthment • Transmembrane channel {porins}13
Protien ll • Opacity associated outer membrane protein OPA • Opaque colonies • A strain may express 3 varients at a time • Clumping of cocci in exudates • LPS • Endotoxin • IGA1 protease RESISTANCE • Delicate, strict parasites • Dies in 2hr outside body • 3-4 days in cultures • Survives in slants at 35 °C if kept under sterile paraffin oil • For years if frozen &left at -70 °C
PATHOGENESIS • Route―› Sexual contact vertical transmission • source ―›carrier; patient • Adhesion is firm ,rapid that micturition after exposure offers no protection • IP ―›2-8 Days • Asyptomatic carriers are seen in women but not in men
CLINICAL FEATURES • In men • Acute urethritis with muco purulent discharge • Extends to prostate, seminal vesicles, epididymis • Chronic urethritis ―›stricture • Periurethral tissues ―›abscess,multiple discharging sinuses {watercan perineum} • In women • Infection to urethra & cervix • Vaginal mucosa is not affected
Extends to Bartholins gland, endometrium, fallopian tubes • PID, Salpingitis―›sterility • Fitz-Hugh-Curtis Sydrome peritonitis with perihepatic inflamation • In both • Proctitis ; women ―›contageous spread men ―›anal sex • Conjunctivitis • Blood invasion ; metastatic lesions ―›arthritis, endocarditis, meningitis • In new born • Gonococcl ophthalmia • bacteremia ―›papules , pustules;tenosinuvitis , suppurative arthritis
EPIDEMIOLOGY • Natural infection ―›humans • Experimentally in chimpanzees • Source –carriers; patients • Route – venereal; fomtes no role • When sulphonamides & penicillins were found for Rx it was hoped to be eradicated • Declined temporarly & rised • One of the most common infective disease • In 1980’s decline with AIDS scare • Higher incidence with blood group B
LABORATORY DIAGNOSIS • Microscopy • Culture • Fluorescent antibody technique • Compliment fixation test • Specimen • Acute case ―›urethral discharge in women cervical also • Chronic case ―›morning drop of secretion exudate after prostatic massage • Centrifused deposits of urine
Intracellular gram negative diplococci in smears is enough for men • Unreliable for women as some normal genital flora has same morphology • Use of fluorescent antibody technique has increased sensitivity & specificity for diagnosis • Culture Specimens should be inoculated on prewarmed plates • If not; collected on charcoal impregnated swabs & sent in Stuart’s transport medium • In acute cases ―› chocolate agar & MHA • In chronic cases as mixed infection is usual Thayer-Martin medium is used • Growth identified by morphology &biochemical reactions