Download
1 / 15
160 likes | 373 Views
Age Related Macular Degeneration. Bethan. Epidemiology. Most common cause irreversible visual loss in >50yrs 10% > 65-74yrs 30% > 75yrs Prevalence increasing with ageing pop White ? women. Aetiology. Age Smoking Pos fhx High BP ? Sunlight ? Alcohol ?obesity

E N D
Epidemiology • Most common cause irreversible visual loss in >50yrs • 10% > 65-74yrs • 30% > 75yrs • Prevalence increasing with ageing pop • White ? women
Aetiology • Age • Smoking • Pos fhx • High BP • ? Sunlight • ? Alcohol • ?obesity • Healthy diet & exercise - protective
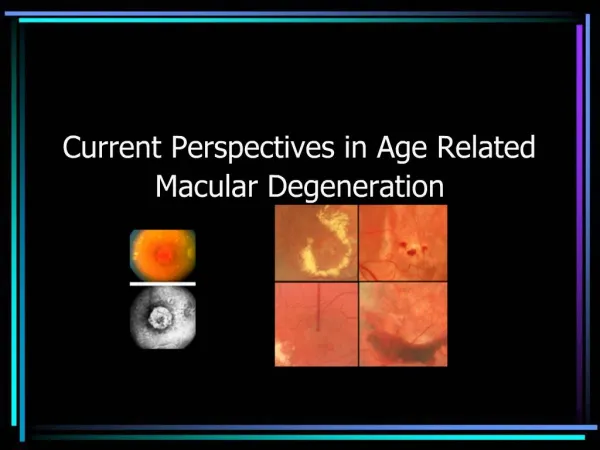
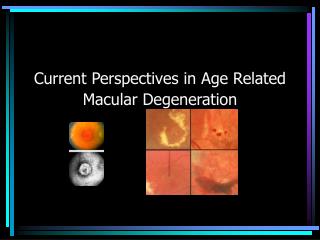
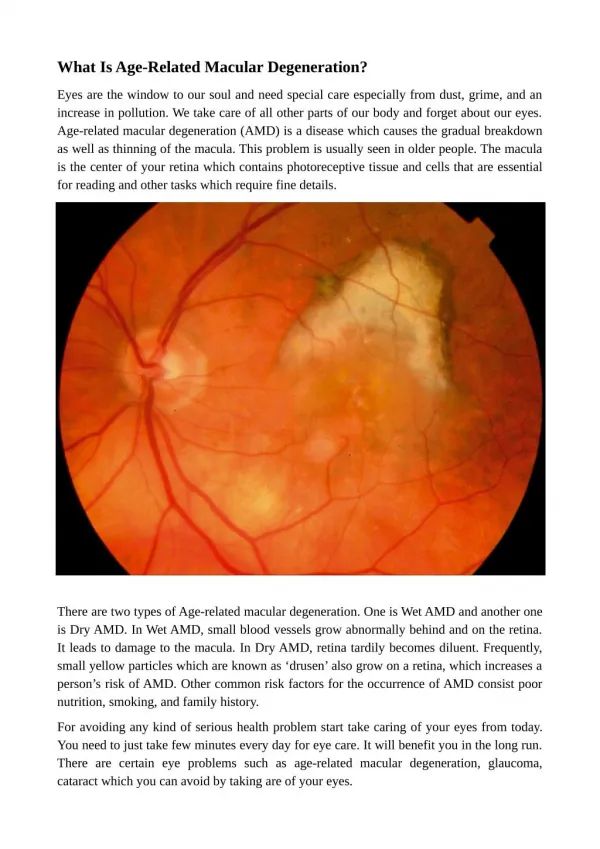
pathogenesis • Deposition of colloid bodies (drusen) in macular area between retinal pigment epithelium (RPE) and underlying (bruch’s) membrane • From age 45 • Age related maculopathy • Critical size/ number – ARMD • Early ARMD – vision preserved (small, apigmentary) • Late ARMD – vision affected (large, pigmented) • Two subtypes
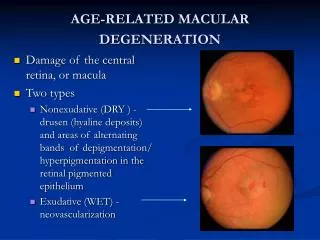
Dry • Atrophic, dry, non exudative, geographic • 90% of cases • Atrophy of neuroretina – • RPE • Photoreceptors (over rpe) • Choriocapillaris (below rpe)
Wet • Wet, exudative, neovascular • 10% of patients • Drusen lift retinal pigment epithelium from blood supply • Choroidal vessal growth – sub retinal neo vasc, (SRNV), retinal angiomatous proliferation • serous fluid accumulation, vessels leak, scars formed
Differential diagnosis • Refractive errors. • Cataracts. • Some corneal diseases. • Posterior vitreous detachment or retinal detachment. • Retinal artery occlusion or retinal vein occlusion. • Central serous retinopathy. • Cerebrovascular disease. • Pituitary and other neurological tumours. • Some drugs or chemicals including methanol, chloroquine, hydroxychloroquine, • Rule out diabetes (diabetic maculopathy). • Type 2 membranoproliferativeglomerulonephritis. • Various rare ophthalmic conditions to be ruled out by ophthalmology team.
Clinical features • Bilateral 1 > loss • Deterioration/distortion of central vision –scotoma – lines, micro/macropsia • Dark patch “shadowy figure” on waking • Visual hallucinations with severe v loss • Incidental at optometrist • Affected adl’s – driving, reading, recognition • Night glare, photopsia, • Sudden deterioration (bleed) +/- floaters
Investigations • Visual acuity • Fundus – yellow deposits • Slit lamp exam • Optical coherence tomography (OCT) • Fluorescein angiography
Referral • Ref ophthalmology –within one week • Or optometrist
Management - support • No effective treatment for dry ARMD • Register blind - ophthalmologist • Social support • Visual rehab – refract to optomise vision, magnify/ telescope, large print books, house aids • Counselling – reassure re peripheral vision, advise about DVLA • Txt of choroidal neovascularisation - criteria
Management –wet ARMD • Laser photocoagulation – away from fovea • Verteporfin – iv injection activated by argon laser beam – stabilises condition • Anti VEGF’s – prevent endothelial cell proliferation – intraocular • PDT & anti VEGF • Surgical options rarely used • Immunomodulation is being explored
ranibizumab • Monoclonal antibody to vascular growth factor • Injected into eye 1/12 x3 • NICE & RCO criteria –minority ok • 80% slows visual loss • Aims to preserve central vision • Complications - Retinal detachment, haemorrhage, infection, hypersensitivity
Advice • See GP if worsening or other eye affected • Stop smoking • ? Prevention... • Healthy diet with antioxidants & carotenoids • High dose vitamin & mineral supplements