Download
1 / 38
380 likes | 715 Views
Warwick Emergency Care and Rehabilitation. 2. NHS Service Delivery And Organisation R

E N D
1. Warwick Emergency Care and Rehabilitation 1
Ambulances and overcrowded emergency departments
Prof Matthew Cooke
Warwick Medical School, UK
Emergency Medicine Advisor,
Government Dept of Health, UK
2. Warwick Emergency Care and Rehabilitation 2 This 14-month project was submitted to and funded by the service delivery organisation with the aim of ��This 14-month project was submitted to and funded by the service delivery organisation with the aim of ��
3. Warwick Emergency Care and Rehabilitation 3
For patients, most important area for improvement - waiting time (Cooke & Jenner, 2002).
Long wait in ED commonest cause of complaints (Trout et al., 2000).
Improving emergency care - UK government priority.
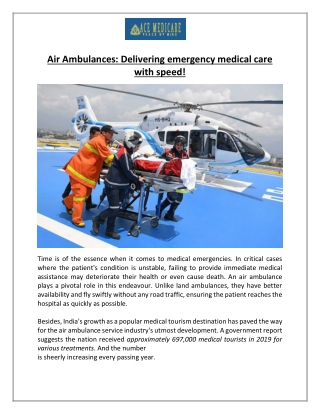
Background Research has shown that for patients the most important area for improvement in emergency departments is waiting time.
Long waiting times in emergency departments is the commonest cause of complaints (Trout et al., 2000).
And improving emergency care is a government priority in the UK.
Research has shown that for patients the most important area for improvement in emergency departments is waiting time.
Long waiting times in emergency departments is the commonest cause of complaints (Trout et al., 2000).
And improving emergency care is a government priority in the UK.
4. Warwick Emergency Care and Rehabilitation 4
ED overcrowding
12 hour waits for admission
4 hour total time in ED
Background Research has shown that for patients the most important area for improvement in emergency departments is waiting time.
Long waiting times in emergency departments is the commonest cause of complaints (Trout et al., 2000).
And improving emergency care is a government priority in the UK.
Research has shown that for patients the most important area for improvement in emergency departments is waiting time.
Long waiting times in emergency departments is the commonest cause of complaints (Trout et al., 2000).
And improving emergency care is a government priority in the UK.
5. Warwick Emergency Care and Rehabilitation 5
Ambulances waiting outside EDs
Decreased response times
Staff morale
Patient care compromised
Background Research has shown that for patients the most important area for improvement in emergency departments is waiting time.
Long waiting times in emergency departments is the commonest cause of complaints (Trout et al., 2000).
And improving emergency care is a government priority in the UK.
Research has shown that for patients the most important area for improvement in emergency departments is waiting time.
Long waiting times in emergency departments is the commonest cause of complaints (Trout et al., 2000).
And improving emergency care is a government priority in the UK.
6. Warwick Emergency Care and Rehabilitation 6 TARGETS AMBULANCE
15 minutes maximum time to handover
CONFLICT WITH
4 hours maximum stay in the ED
7. Warwick Emergency Care and Rehabilitation 7 Missing the point Example
When more than 4 ambulances are waiting to handover patients, then an ambulance officer will be allocated to care for these patients in the corridor to free up the other crews
?? Patient centred solution??
8. Warwick Emergency Care and Rehabilitation 8 Systematic Review according to guidelines from NHS Centre for Reviews and Dissemination
Search strategy - 61860 studies.
Initial sift of titles and abstracts - 3178
334 were fully reviewed
109 met the selection criteria.
Method The search strategy generated a total of 61860 studies.
Following the initial sift the tilites and abstracts of 3178 were reviewed and of these 334 were fully reviewed, and
109 met the selection criteria.
The search strategy generated a total of 61860 studies.
Following the initial sift the tilites and abstracts of 3178 were reviewed and of these 334 were fully reviewed, and
109 met the selection criteria.
9. Warwick Emergency Care and Rehabilitation 9 Background Call prioritisation
evidence of safety is poor (Wilson, 2002)
up to 30% error rate (Cooke 1999, Nicholl 1996)
30-52% do not require emergency ambulance (Snooks, 1998)
Most are transported to ED
10. Warwick Emergency Care and Rehabilitation 10 Possible solutions Divert non serious 999 calls to Nurse Advice
Ambulance crew treat and discharge
Ambulance crew choose most appropriate destination
11. Warwick Emergency Care and Rehabilitation 11 Divert calls to Nurse Advice 52% triaged as not requiring emergency ambulance and a third of these did require ED. BUT 9% of those triaged as not requiring ambulance were admitted to hospital (Dale 2003)
US study showed 98% negative predictive value for ED attendance
12. Warwick Emergency Care and Rehabilitation 12 Divert calls to Nurse Advice NHS Research � soon to be published
13% of all 999 calls
67% returned, of which 25% needed 999
Callers satisfied
Adverse events 4 in 1552
13. Warwick Emergency Care and Rehabilitation 13 Standard ED triage cannot be used
AMPDS not designed for this (26% of non transports were delta)
14. Warwick Emergency Care and Rehabilitation 14 Different Destination London- extra protocols introduced for transport to MIU. No change in turnaround times, no decrease in ED usage. (LAS 2002)
London - treat and refer protocols. No change in conveyance to hospital; 6 minutes longer cycle time; 9% of those left at home were admitted within 14 days (Snooks, 2001)
15. Warwick Emergency Care and Rehabilitation 15 3% had critical incident when paramedic thought appropriate to leave at home and 11% potential incidents(Schmidt, 2000)
9.6% undertriage, half due to guideline violations. 8.4% incorrectly stated not to need ED. (Pointer 2001)
22% of non transported were inappropriate (Selden 1991)
16. Warwick Emergency Care and Rehabilitation 16 Alberquerque study suspended. (1998)
Low agreement between paramedics and ED physicians on need for ED care (Hauswald 2002)
32% of those determined by paramedic to not need treatment were deemed incorrect (Silvestri 2002)
17. Warwick Emergency Care and Rehabilitation 17 Limitations International variation
Training given for role
Short time series
Expert opinion rather than actual outcome
18. Warwick Emergency Care and Rehabilitation 18 Conclusions from Literature Safety is not confirmed for these changes and doubts have been raised
Should proceed with caution
Full evaluation is required
19. Warwick Emergency Care and Rehabilitation 19 WORKING TOGETHER Access to data
Combined escalation plans
Neutral Referee
20. Warwick Emergency Care and Rehabilitation 20 CAPACITY MANAGEMENT Control flows
Spreading the workload
Which patients
When to start
Problems
21. Warwick Emergency Care and Rehabilitation 21 DIVERSIONS Recognised as bad for patients (Schull 2004)
What benefit?
Can create artificial variability in a system
Variation creates poor performance
22. Warwick Emergency Care and Rehabilitation 22 DIVERSIONS Should be for exceptional circumstances
If used regularly suggests failure to use predictive analysis and failure to plan
23. Warwick Emergency Care and Rehabilitation 23 Early intervention, not waiting until the crisis
EDs can tell you several hours in advance of the �crisis�
24. Warwick Emergency Care and Rehabilitation 24 DIVERSIONS Should be last resort
REMEMBER
Different from planned bypass
25. Warwick Emergency Care and Rehabilitation 25 BYPASSING THE ED Obvious admissions obviously need admitting
So why do they have to go through the emergency department
26. Warwick Emergency Care and Rehabilitation 26 What is the role of the ED?
27. Warwick Emergency Care and Rehabilitation 27 NOTHING DIFFERENT Why do something different when it is busy?
If it is best for patient when it is busy�..?
28. Warwick Emergency Care and Rehabilitation 28 DECREASING VARIABILITY Smoothing the workload
GP urgent transfers at lunchtime
Flexible catchment areas
29. Warwick Emergency Care and Rehabilitation 29 Ambulance Solutions are long term Help reduce attendances
Not a fire fighting measure
30. Warwick Emergency Care and Rehabilitation 30 Ambulance turnaround delays Getting ownership
Not an ambulance solution!
BUT�.
31. Warwick Emergency Care and Rehabilitation 31 Essex Ambulance Action when turnaround times increased
Help get patients out of hospital
Unclog the system
32. Warwick Emergency Care and Rehabilitation 32 The main solution = ED performance
33. Warwick Emergency Care and Rehabilitation 33 THE solution to diversion ALL EDs accept patients all the time
All Hospitals accept patients from ED
All Homes accept discharges
www.warwick.ac.uk/go.edwaits
34. Warwick Emergency Care and Rehabilitation 34 Freeways Find the bottleneck
Don�t just make bigger roads and more vehicles
35. Warwick Emergency Care and Rehabilitation 35 GETTING TO THE SOLUTION Patient�s perspective
Eliminating artificial barriers between healthcare organisations
36. Warwick Emergency Care and Rehabilitation 36 The future of ambulance services Why do we need ambulance services as a separate entity?
One emergency healthcare service
37. Warwick Emergency Care and Rehabilitation 37 One final thought Local solutions are best
But hopefully some of the UK experience will be helpful
38. Warwick Emergency Care and Rehabilitation 38 Reducing ED attendances - can ambulance services help?
Prof Matthew Cooke
Warwick Medical School, UK
www.warwick.ac.uk/go/ambulance
.
.