Download
1 / 39

E N D
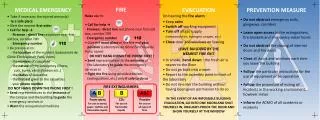
A medical emergencyis an injury or illness that is acute and poses an immediate risk to a person's life or long term health. Dependent on the severity of the emergency, and the quality of any treatment given, it may require the involvement of multiple levels of care, from a first aider to an emergency physicianthrough to specialist surgeons. • Any response to an emergency medical situation will depend strongly on the situation, the patient involved and availability of resources to help them. It will also vary depending on whether the emergency occurs whilst in hospital under medical care or in the street or alone at home).
Circulatory emergency: • The heart & blood vessels (circulatory & CVS) work constantly to keep all parts of the body supplied with blood, carrying oxygen & nutrients. • The circulatory system can fail for 2 main reasons: Severe bleeding & fluid lossmay cause blood volume to fall & deprive vital organs (brain, heart & lungs) of oxygen Age & diseasecan cause the body’s circulatory system to break down.
Aim of management: • To improve blood supply to the heart & brain. • In minor incidents (fainting) appropriate first aid ensure recovery. • In serious cases (heart attack) your role may be vital in preserving life until medical aid arrives.
First aid priorities: • Position the casualty to improve the blood supply. • Take additional measures to improve circulation & breathing. • Comfort & reassure the casualty (fear & panic will put extra strain on the heart). • Obtain appropriate medical assistance.
Shock: • Tissues don’t receive adequate blood supply to provide necessary O2 & nutrients leading to cellular death, organ failure and death.
The circulatory system distributes blood round the body, so that O2 & nutrients can pass through & perfuse tissues. • When the system fails, circulatory shockwill develop. If not treated, vital organs (heart & brain) may fail leading to death. • If there is risk of shock, reassuring the casualty & making him comfortable may be sufficient to prevent the condition to deteriorate (Shock is made worse by fear and pain).
Causes of Shock • Shock can develop when the heart pump fails to work properly, causing a reduction in the pressure of the circulating blood. The most common cause of this type of shock is a heart attack. • Shock can develop as a result of a reduction in the volume of fluid circulating around the body. external or internal bleeding, or loss body fluids through severe diarrhoea, vomiting, or burns. The blood supply is diverted from the surface to the core of the body. The main symptoms and signs of shock relate to such redistribution of the circulation.
There are 3 main types of shock: hypovolaemic, cardiogenic and vasogenic shock. • In hypovolemic shock, the problem is that there is a loss of fluid from the circulation. • In cardiogenic shock, there is a failure of the pump, although the blood volume is not affected. • While in vasogenic shock, the blood volume is again not affected but rather the arterioles and capillaries dilate, leading to diminished venous return and hence diminished cardiac output leading to decreased tissue perfusion i.e. shock.
Classification of Shock by Cause: • Hypovolaemic: • Hemorrhagic: blood loss due to soft tissue bleeding, fractures, wounds, …… etc. • Burns: loss of plasma in burn exudates. • Dehydration: major body fluid loss, e.g. due to prolonged vomiting, diarrhea or metabolic disorders as diabetic ketoacidosis.
Cardiogenic • Failure of cardiac pump leading to inadequate cardiac output e.g. after myocardial infarction. • Vasogenic • Septic:endotoxins from G-ve bacteria can cause massive vasodilatation in certain infective conditions. • Anaphylactic: severe allergic reaction, histamine release leads to dilatation of capillaries and arterioles. • Neurogenic: loss of sympathetic control leading to dilatation of venules, capillaries and arterioles.
Symptoms progression: • Release of adrenaline causes: Rapid pulse, Sweating, small vessels in non vital areas ,as the skin, shut down to divert blood & O2 supply to vital organs (pale, cold & blue skin). • As shock develops: Weakness, Nausea & vomiting, Thirst, Rapid, Shallow Breath & Weak Pulse. • As the brain’s O2 supply weakens: Restlessness, anxiety & aggressiveness, Air hunger, Undetectable pulse, Unconsciousness & finally Heart stops
Symptoms: • Pale, cool and clammy (moist) skin. • Hypotension with tachycardia • Irregular respiration & Chest pain. • Confusion or loss of consciousness (up to coma). • Pupils may be dilated. • Renal failure and diminished urine output. • Diarrhea (large intestine becomes irritated due to hypotension).
Your aims are: • To recognize shock. • Treat any obvious cause. • Improve blood supply to the brain, heart & lungs. • Arrange removal to hospital.
Treat any cause of shock (external bleeding) • Lay the casualty down • Raise & support legs to improve blood supply • Loosen tight clothing (to reduce constrictions at the neck, chest & waist) • Keep casualty warm • Check & record breathing & pulse (CPR if necessary)
First Aid Management: • Assess the ABCs & begin CPR (if needed). • Call EMS. • Have the person lie down on his back with feet higher than head (head down position) . • Keep the person warm & comfortable. • Give nothing by mouth (even if thirsty). • If person vomits or bleeds from the mouth, turn him on his side. • In case of bleeding, try to control it by pressure.
Have the person lie down on his back with feet higher than the head(head down position)). “This will force blood to go to the thorax, increasing venous return to the heart and hence increasing cardiac output”
First Aid Management (cont.): • Further management depends on cause: • Blood transfusion in bleeding. • IV fluids in dehydration. • Dopamine in cardiogenic shock. • Atropine in neurogenic shock.
Treatment of Shock • Treat any cause of shock which can be remedied (such as external bleeding). • Lay the casualty down, keeping the head low. • Raise and support the casualty’s legs (be careful if suspecting a fracture). • Loosen tight clothing, braces, straps or belts, in order to reduce constriction at the neck, chest and waist. • Insulate the casualty from cold, both above and below. Contact the emergency service. • Check and record breathing, pulse and level of response. Be prepared to resuscitate the casualty if necessary.
DO NOT let the casualty move unnecessarily, eat, drink, or smoke. • DO NOT leave the casualty unattended. Reassure the casualty constantly.
Impaired Consciousness: • Unconsciousness is a serious state which may cause anxiety and worry to the first aider. However, prompt efficient action which secures a good airway and removes any obstruction such as blood, vomit or dentures may prevent complications and save life of the patient. The patient becomes unconscious as the immediate result of any injury or a disease affecting the CNS.
Depth of unconsciousness: • Lucid: the patient is cooperative and conscious. • Confusion: he is disorganized but will obey commands. • Semi-coma: the patient will only react to painful stimuli but not voice commands; unconscious. • Coma: there is no response to stimuli; deeply unconscious.
This results from an interruption of the brain’s activity. Whatever the cause, follow these 3 rules: • Ensure the airway is clear • Keep checking response level “AVPU” code Alert, responds to Voice, responds to Pain, Unresponsive time. Assessing level of response (GLASGOW COMA SCALE) eyes, movement, speech.
Causes of impaired consciousness: • Cerebrovascular accident: bleeding from a cerebral blood vessel leading to intracerebral hemorrhage. Alternatively, there may be occlusion of a blood vessel due to a thrombus. • Fits:(idiopathic epilepsy) In grand mal epilepsy, the patient goes into tonic period of some 30 seconds or so when patient's musculature goes into spasm and the patient is unable to breath, this is followed by the clonic stage of convulsions which passes into a deep coma from which the patient gradually wakes up.
Diabetes:in hyperglycemic states, increased lipolysis leads to the formation of ketones whose effects on the brain lead to unconsciousness. In hypoglycemic states, the lack of blood glucose affects brain to produce drowsiness, confusion and unconsciousness. • Acute infections and toxaemic states: any infections involving the brain, any infections leading to hypoxia (chest infections) as well as toxaemic states as uraemia.
Fainting: • Person is unable to respond to external stimuli & unaware of his surroundings. • Last from seconds to minutes. • ↓ Blood flow or glucose supply to the brain.
Fainting occurs when the blood supply to your brain is momentarily inadequate, causing you to lose consciousness. This loss of consciousness is usually brief. • Fainting can have no medical significance, or the cause can be a serious disorder. Therefore, treat loss of consciousness as a medical emergency until the signs and symptoms are relieved and the cause is known.
Unlike shock, the pulse becomes very slow, although it soon picks up & returns to normal. Recovery from faint is usually rapid & complete. • A faint may be a reaction to pain or fright, emotional upset, exhaustion or lack of food. • It is common after long periods of physical inactivity (standing still) especially in a warm atmosphere. The inactivity causes blood to pool in the lower part of the body, reducing the amount of O2 available to the brain.
Recognition: • A brief loss of consciousness causing the casualty to fall to the floor. • A slow pulse • Pale, cold skin and sweating.
Causes: • Low blood sugar (hypoglycemia) e.g. in diabetics, in early pregnancy, in persons on severe diets, etc. • Anemia. • Conditions which cause rapid blood loss. • Abnormal heart rhythm or heart attack. • Stroke. • Head injury or concussion. • Heat stroke or heat exhaustion. • Hypoxia.
Other causes of fainting include: • Poisoning. • A sudden change in body position like standing up too fast (postural hypotension). • A side effect of some medications. • Drinking too much alcohol. • Anxiety or sudden emotional stress or fright. • Being in hot, humid weather or in a stuffy room. • Standing a long time in one place. • Extreme pain.
First Aid Management: • Check for ABC, provide CPR and treat for shock as needed. If you feel faint • Lie down or sit down. To reduce the chance of fainting again, don't get up too quickly. • Place your head between your knees if you sit down.
If someone else faints: • Position the person on his or her back.If the person is breathing, restore blood flow to the brain by *raising the person's legs above heart level about 30 centimetres . *Loosen belts, collars or other constrictive clothing. To reduce the chance of fainting again, *don't get the person up too quickly. If the person doesn't regain consciousness within one minute, call EMS. • Check the person's airway to be sure it's clear. Watch for vomiting. • Check for signs of circulation (breathing, coughing or movement). If absent, begin CPR. Call your local emergency number. Continue CPR until help arrives or the person responds and begins to breathe.
Check for a medical alert tag or drug. • Exclude hypoglycemia as a cause. • Further treatment depends on the cause. • In epileptic fits, prevent victim from endangering himself & when fits stop put him in recovery position.
Don't give the person anything to eat or drink, not even water. • Don't slap or shake a person. • If the person was injured in a fall associated with a faint, treat any bumps, bruises or cuts appropriately. Control bleeding with direct pressure.