Download

1 / 28
290 likes | 343 Views
Explore the survival and efficacy of natural antiplatelets and anticoagulants against synthetic counterparts like Heparin and Aspirin. Learn about atherothrombosis, drug targets, mechanisms of action, and milestone developments in anticoagulation and antiplatelet therapy. Discover how newer oral anticoagulants compare to traditional agents and their advantages. Delve into the future outlook of Warfarin and related oral anticoagulants in managing thromboembolic disorders.

E N D
Natural versus Synthetic Anticoagulants and Aniplatelets in Thromboembolic Disorders Principles & Practice Shaker Mousa, PhD, MBA, FACC, FACB Professor of Pharmacology & Chairman of PRI, Albany, NY, USA
Would the Natural Antiplatelet and Anticoagulants Survive the Challenge of the Synthetic Ones? Would Heparin Survive the Challenge? Would Aspirin Survive the Challenge? Would Warfarin Survive the Challenge?
Co-morbidity of Atherosclerotic Disease a major health burden • Atherothrombosis • major complications of atherosclerosis are thrombosis, with local occlusion or distal embolization CAD CVA PAD At PRI: We are advancing functional HDL elevating mechanisms (EL inhibitors) & LDL Lowering mechanisms by inhibiting PCSK9
Atherothrombosis & Risk Factors for CHD Blood cholesterol10% = 20%-30% in CHD High blood pressure5-6 mm Hg = 42% in Stroke = 16% in CHD Cigarette smokingCessation = 50%-70% in CHD Body weight BMI<25 vs BMI>27 = 35%-55% in CHD Physical activity20-minute brisk walk daily = 35%-55% in CHD
Antiplatelet Drug Targets TRA Platelet Thrombin PAR-1 Platelet PAR - 1 Fibrinogen PAR-4 Clopidogrel Prasugrel Ticagrelor P2Y1 GP IIIa ADP GP IIb P2Y12 P2Y12 GP IIb Thromboxane A2 Aspirin TXA2-R GP IIIa Epinephrine Serotonin 5HT2A Gp IIb/IIIa inhibitors Anionic phospholipid surfaces GP VI Collagen GP Ia
Milestones For Aspirin 5th century BC Hippocrates 1897 AD Felix Hoffman/Friedrich Bayer 1900 – present Most widely used drug in the world 1971 Sir John Vane
Aspirin: Mechanism of Action Membrane Phospholipids Arachadonic Acid Aspirin COX-1 Prostaglandin H2 Thromboxane A2 Platelet Aggregation Vasoconstriction Prostacyclin Platelet Aggregation Vasodilation
Aspirin Impact on CVD • Aspirin in the treatment of CVD • Additive benefits of aspirin and statins • Aspirin in the prevention of CVD • Dual antiplatelet therapy in CVD • Newer antiplatelet agents in CVD
Aspirin Evidence: Dose and Efficacy Indirect comparisons of aspirin doses on vascular events in high-risk patients Odds Ratio for Vascular Events Aspirin Dose No. of Trials (%) 500-1500 mg 34 19 160-325 mg 19 26 75-150 mg 12 32 <75 mg 3 13 Any aspirin 65 23 P<.0001 0 0.5 1.0 1.5 2.0 Antiplatelet Better Antiplatelet Worse Antithrombotic Trialist Collaboration. BMJ 2002;324:71-86
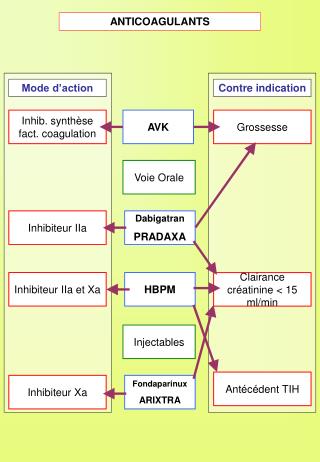
1998Firstcommercially available direct anti-thrombin (DTI) 2001First commercially available synthetic factor Xa inhibitor 1993First commercially available LMWH 1916 -1940sHeparin commercially available I N J E C T A B L E A G E N T S 55 Years 2010-2013First oral direct anti-IIa anti-Xa 2009First oral direct anti-Xa 1954Warfarin commercially available Advances in Anticoagulation 1940 1950 1960 1970 1980 1990 2000 2010 O R A L A G E N T S *United States
Warfarin: Mechanism of Action Vitamin K Antagonism of Vitamin K VII Synthesis of Non- Functional Coagulation Factors IX X II Warfarin Ansell J et al. Council on Clinical Cardiology. www.americanheart.org
Adjusted Odds Ratios for Ischemic Stroke and Intracranial Bleeding in Relation to Intensity of Anticoagulation 15.0 Intracranial Bleed Stroke 10.0 Odds Ratio 5.0 1.0 0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 INR Fuster et al. J Am CollCardiol. 2001;38:1231-1266.
Conversion from Heparin to Warfarin in VTE • May begin concomitantly with heparin therapy • Heparin should be continued for a minimum of four days • Time to peak antithrombotic effect of warfarin is delayed 96 hours (despite INR) • When INR reaches desired therapeutic range, discontinue heparin (after a minimum of four days). • Certain indications favor LMWH alone vs. Warfarin
Xa Common Pathway New Oral Agents Xa Blocker Apixaban Rivaroxaban Edoxaban Dabigatran Prothrombin Thrombin Clot Fibrin Fibrinogen
? ? ? • Cheap ?
Chemical structure of various oral anti-Xa agents Edoxaban TAK 442 Apixaban LY 517717 Betrixiban Rivaroxaban
Chemical Structure of Warfarin, Tecafarin and Oral Anti-II Agents Warfarin Ximelagatran Discontinued Dabigatran Tecarfarin
Newer Oral Anticoagulants: Advantages • Immediate onset of action • Fixed dose • No laboratory coagulation monitoring • Minimal drug-drug/ drug-food interactions • Many indications: VTE prevention/ Rx, Stroke Prevention in AF • Short half-life; therefore, no “bridging”, Patients at risk if forgot taking the dose
Future of Warfarin and Related Oral Anticoagulants (Coumarin Derivatives) • Excellent efficacy • Low Cost ($0.75 per day!) • Long Track Record (1954) • Centralized Anticoagulation Clinics • Point-of-care testing • Clinical history and reliability • The patient will not be at risk of thrombosis if missed doses unlike NOA
Glycosaminoglycans: Heparins, LMWH, and Non-Anticoagulant Heparin Beyond Anticoagulation • Anti-Inflammatory • Anti-Complement • Anti-Adhesive • Anti-Angiogenesis • Anti-Cancer • Anti-Metastasis
Angiogenesis Supports Tumor Growth & Metastasis Micro-Environment • Inflammation • Pro-thrombotic State Vascularization Metastasis
Anti-Angiogenesis Effect of Camel GAGs (Urine) in the VEGF/FGF2-stimulated Angiogenesis in the CAM Model FGF/VEGF Control FGF/VEGF+ NACH FGF/VEGF+ LMWH FGF/VEGF+ GAG
Would the Natural Antiplatelet and Anticoagulants Survive the Challenge of the Synthetic Ones? Would Heparin Survive the Challenge? Would Aspirin Survive the Challenge? Would Warfarin Survive the Challenge?