Download
1 / 23
230 likes | 242 Views
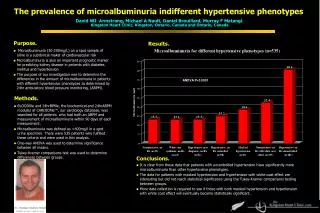
This study explores the prevalence and case fatality of cardiac phenotypes among infants with Down syndrome. The research examines various cardiac defects and mortality rates, shedding light on the importance of congenital heart defects for survival among children with Down syndrome.

E N D
Prevalence and Case Fatality of Cardiac Phenotypes among Infants with Down Syndrome MCH EPI Conference, Atlanta, 2007 M Shin, JE Kucik, T Riehle-Colarusso, A Correa
Down syndrome (DS) Epidemiology • Birth prevalence: 1 in 800 live births • Trisomy 21 • Survival probability: 92.9% survival probability to 1 year, 88.6% survival probability to 10 years (Rasmussen et al, Survival in Infants with Down Syndrome, Metropolitan Atlanta, 1979-1998)
Down syndrome (DS): Overall • Dysmorphic facial • features • Hand and foot • anomalies • Mental retardation • Delayed maturation • and growth • Subfertility/sterility • Hypothyroidism • Hearing Loss • Eye disease • Heart defects
Down Syndrome: Cardiac All types: 40% AV Canal “family” 40% Complete AVC Primum-type ASD VSD, all typesASD,secundum PDA Tetralogy of Fallot
Study Background • Congenital heart defects (CHD) are an important prognostic factor for survival among children with Down syndrome (DS). • Information on the population-based prevalence and case fatality rate (CFR) of cardiac phenotypes among infants with DS is limited.
Study Questions • What is the prevalence of various cardiac phenotypes among infants with DS? • What are the ratios of case fatality rates for the various cardiac phenotypes among infants with DS compared to those without CHD?
Methods • Infants with DS born from 1979 - 2003 were identified from a population-based birth defects registry, Metropolitan Atlanta Congenital Defects Program (MACDP). • Death status among infants with DS through December 31, 2004 was identified from MACDP records, Georgia vital records, and a probability-based linkage with National Death Index (NDI)1 Wong, LY, Paulozzi, L. 2001. Survival of infants with spina bifida: a population study 1979-94. Peditri Perinata Epidemiol, 15:374-378.
Methods • All records with CHD were reviewed and classified according to a clinical nomenclature adopted from the Society of Thoracic Surgeons (STS)1 • CHD in DS infants were then grouped as: • Isolated • Multiple (more than one CHD) • Common Associations: AVSD+ASD, ASD+VSD, AVSD+PDA • Other association 1Riehle-Colarusso et al, (2007) Improving the Quality of Surveillance Data on Congenital Heart Defects in the Metropolitan Atlanta Congenital Defects Program, BDRA
Methods • Prevalence of DS with CHD for each cardiac phenotype was estimated (per 100 live births with DS). • Case Fatality Rates (CFRs) for each cardiac phenotype were compared with the CFR for DS infants without CHD using ratios of CFR. • Mantel-Haenszel method and 95% Confidence Interval (CI).
Results • Total DS cases : 1027 live births • Total DS cases with CHD : 416 cases (40.5%) • Total number of CHD: 526 (case can have more than one CHD)
Proportion of CHD among infants with DS, 1979-2003, metropolitan Atlanta Chi-Square p=0.37
RVOTO 1% LVOTO 2% OTHERS 1% CONOT 4% PDA 9% AVSD 37% ASD 20% VSD 26% Cardiac phenotypes among infants with DS and CHD (n=526) PDA=patent ductus arteriosus, CONOT=Conotruncal, LVOTO=left ventricular outflow tract obstruction, RVOTO=Right ventricular outflow tract obstruction
Case Fatality Rates by Cardiac Phenotype among Infants with DS, Isolated Heart Defects
Case Fatality Rates by Cardiac Phenotype among Infants with DS, Multiple defects - Common associations
Case Fatality Rate by Cardiac Phenotype among Infants with DS, Multiple defects - other association
Adjusted Ratios* of Case Fatality Rates *adjusted for birth weight, sex and race/ethnicity
Conclusion • 40.5% of infants with DS were found to have CHD; The most frequent CHD was AVSD (33.4%). • The presence of CHD is associated with a two-fold higher risk of dying within one year compared to those without CHD. • Infants with DS and either an isolated CHD or other associated multiple CHD have a higher risk of mortality compared to those without CHD.
Conclusion • Higher mortality predominantly due to presence of AVSD, either in isolation or combined with other heart defects. • Classification of specific cardiac phenotype among DS with CHD can contribute to the understanding of factors associated with higher mortality.
Next Steps • Further Analysis on the severity of the heart defects (AVSD) • Further analysis of children with AVSD without Down syndrome
Thank You Picture from http://www.nads.org/