Download
1 / 18
180 likes | 192 Views
Explore exercises and treatments for spinal issues like scoliosis, lordosis, kyphosis, and rounded shoulders. Learn how to strengthen muscles and improve posture for a healthier back.

E N D
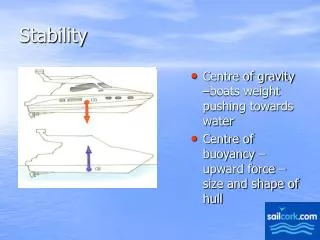
V.C. Muscular Stability • Abdominal muscles on ventral side: 1. Prevent V.C. hyperextension 2. Pull pelvis toward sternum 3. Pull thorax toward pelvis • Erector Spinae muscles on dorsal side: 1. Compress V.C. 2. Holds V.C. together
CONTRALATERAL Trunk Flexion moving trunk away from “throwing” armFIG 7.4page 233
IPSILATERAL Trunk Flexion moving trunk towards the “throwing” arm “UNDERARM” Throw Pattern
LORDOSIS • Pelvis tilted towards anterior • often due to weak abdominal muscles • treatment: 1. stretch hip muscles [extensors and flexors] 2. strengthen abdominals and hip flexors
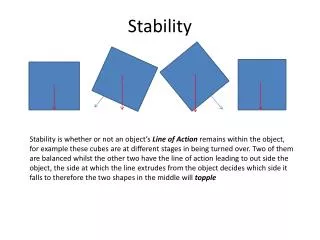
SCOLIOSIS • mediolateral curvature of V.C. [“S” curve] • often caused by one leg shorter than other • treatment of functional problem: 1. Stretch Concave side ) interior of curve 2. Strengthen Convex side ) exterior of curve
KYPHOSIS • exaggerated curve of V.C. anterior/posterior • bending forward of thoracic area along with flattening of lumbar curve • treatment: 1. Strengthen V.C. extensors 2. Stretch V.C. flexors [thoracic area]
Rounded Shoulders • Treatment: 1. Strengthen retractors of shoulder girdle 2. Stretch protractors of shoulder girdle
move vertebral column if pelvis isfixed or stabilized move pelvisif vertebral column is fixed or stabilized move thighsif pelvis is fixed/stabilized move pelvisif thighs are fixed/stabilized SIT UPSAbdominalsHip Flexors
Long Lying Sit-Up: FIG 7.6a page 237 • If Abdominals are Strong: • Abdominals are the prime mover • Abdominals ALONE flex the Vertebral Column • Hip Flexors stabilize pelvis (H.F.do not flex V.C.)
Long Lying Sit-Up: FIG 7.6a • If Abdominals are WEAK: • Abdominals alone cannot flex V.C. (Abs only assist) • Hip Flexors are the prime movers • Hip Flexors pull pelvis and lumbar disks compress
“Leg Lifts”: FIG 7.6b If Abdominals are WEAK: • Abdominals cannot stabilize pelvis (prevent flexing) • Pelvis flexes due to pull of Hip Flexors • Lower Back hyperextends, lumbar disks compress • This exercise requires very strong abdominals
“Bent Leg or Curl” Sit-Up: FIG 7.6c • Hip Flexors are shortened (Length/Tension principle) • H.F. stabilize pelvis (do not flex pelvis) • Abdominals must do most if not all of the work • minimizes hyperextension of lumbar vertebrae
“Snap-Up”: FIG 7.6d • simultaneous Hip and V.C. flexion • requires Torque from Abdominals in 2 ways:1. flexion of the Vertebral Column 2. stabilize Pelvis to prevent it rotating forward
Bent Leg “Curl” Sit Up on Incline BoardFIG 7.6e page 237 • incline position allows resistive Tg to have ROM • depending on of board, Tg may never reach 0
“CRUNCH” SIT-UPNon-Supported Supported More difficult Less difficult from KIN 300/301 Exercise Book by Natascha Weschpage 48
“CRUNCH” SIT-UP: non-supported • Stabilizers activated • Pelvis “flat” or tilted forward • no V.C. hyperextension
Lumbar HYPERFLEXION FIG 4.18a page 163 FIG 4.16c page 161
Lumbar HYPEREXTENSION FIG 7.9 page 242 FIG 7.10page 242