Download
1 / 40
410 likes | 843 Views
2008 Seminar Series Measuring and Analyzing Health Outcomes I-Chan Huang, PhD Lecture 2 Measurement Instrument and Method for Health Outcomes Research Department of Epidemiology & Health Policy Research University of Florida College of Medicine September 29, 2008 Announcement / Q&A

E N D
2008 Seminar Series Measuring and Analyzing Health Outcomes I-Chan Huang, PhD Lecture 2Measurement Instrument and Method for Health Outcomes Research Department of Epidemiology & Health Policy ResearchUniversity of Florida College of MedicineSeptember 29, 2008
Announcement / Q&A • Syllabus, reading materials and PowerPoint • Course website: www.ehpr.ufl.edu/maho • Use your username and password • Q&A • How can I learn about data management and analysis (e.g., software and statistical code) from this seminar series? • How can this seminar series help me address the research questions I encountered?
Outline • Important domains of HRQOL/QOL • Measurement Instrument • Measurement Method • Note: • Only some instruments will be introduced in today’s • seminar. Please contact ICH if you need information • about other instruments and measurement methods. • Will introduce “Measurement Theory” on Oct 25.
Development of PRO/HRQOL instruments Fig 1: Generic instruments Fig 2: Condition-specific instruments McHorney CA, Annu Rev Public Health 1999, pp. 309
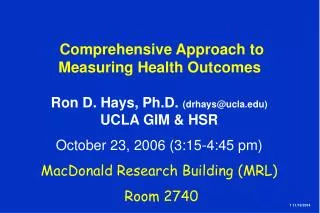
Health outcomes Health Profile Health states and impact on daily functioning and well-being Health Utility A global value of health states Generic measure Disease- or condition-specific measure Direct measure Indirect measure SF-36 WHOQOL-100 MOS-HIV EORTC QLQ TTO SG EQ-5D HUI-3 Type of health outcomes instrument
Domain of HRQOL/QOL outcomes • No consensus on • Specific domains to be measured • Consensus on • A multi-dimensional concept • Agreement on primary and additional domains [Berzon R. Qual Life Res 1993] • Experts’ recommendations from a conference • Primary domains: universally important to all diseases or conditions • Additional domains: important to specific diseases or conditions
Primary domains of HRQOL/QOL • Physical functioning • Ability to perform daily physical activities • Psychological functioning • Level of emotional-welling, e.g., anxiety, depression, guilt and worry • Social functioning • Ability to interact with family, friends and the community • Perception of health status • Self-report of health, which may be different from health status rated by clinicians and significant other • Overall life satisfaction • Perception of overall sense of well-being
Additional domains of HRQOL/QOL • Neuropsychological / cognitive functioning • Memory, recognition, spatial skills, motor coordination • Intimacy and sexual functioning • Type, frequency, satisfaction with sexual activity • Pain • Important for cancer patients or patients with chronic conditions • Symptoms • Severity, frequency, and extent to which impacts daily functioning • Sleep disturbance • Sleep patterns and restorativeness of sleep • Spirituality • Spiritual beliefs and religious values in everyday lives and the ways of coping • Personal productivity
Generic instrument – MOS SF-36v2 • Development • John E. Ware, Jr (MOS SF-36v1; 1992) • From 116 items of the RANDMedical Outcomes Study (MOS) • 8 domains (36 items: 35 +1) • Physical functioning (10 items) • Role limitations due to physical problems (4 items) • Bodily pain (2 items) • General health perceptions (5 items) • Vitality (4 items) • Social functioning (2 items) • Role limitations due to emotional problems (3 items) • Mental Health (5 items) • Other: health transition (1 item) – not used for scoring • Response category • Likert type: 3, 5, or 6 categories
Generic instrument – MOS SF-36v2 (Cont’d 1) Ware JE. 1998, J CLin Epidemiol
Generic instrument – MOS SF-36v2 (Cont’d 2) Ware JE. 1998, J CLin Epidemiol
Generic instrument – MOS SF-36v2 (Cont’d 3) • Alternative forms • SF-12 and SF-8: allowing two summary scores only • RAND-36 and RAND-12: matter of scoring methods • National norm • Comparing the impact of different disease groups on HRQOL outcomes • International projects (IQOLA) • 103 language versions • For international comparison, recommend the use of factor loadings derived from US norm as a standard to calculate domain score of different cultural groups
Generic instrument – WHOQOL-100 • Development • WHOQOL Group (1993) • Allowing the inclusion of national-specific items • 6 domains (24 facets and 100 items) • Physical health (3 facets; 12 items) • Psychologicalhealth (5 facets; 20 items) • Level of independence (4 facets; 16 items) • Social relationship (3 facets; 12 items) • Environment (8 facets; 32 items) • Spirituality, religiousness & personal beliefs (1 facet; 4 items) • Other: overall QOL and general health (4 items) • Response category • Likert type: 5 categories • Language versions: 42 • Alternative form: WHOQOL-BREF and WHOQOL-8
Motivations Whether the same domain (e.g., physical functioning) in the SF-36 and WHOQOL-BREF measure the same construct or not? Methods Factor analysis Relative validity using different anchors: chronic conditions, health care utilization, and a global rating of QOL Conclusions The SF-36 and WHOQOL measures different construct The SF-36 measures the impact of disease / treatment on daily functioning The WHOQOL measures general satisfaction with life The same type of instrument may measure different construct[Huang IC, Qual Life Res 2006]
* Using principal component method with eigenvalue >1.0. ** Communality: proportion of a variable’s variance explained by a factor structure The same type of instrument may measure different construct[Huang IC, Qual Life Res 2006] (Cont’d 1)
The same type of instrument may measure different construct[Huang IC, Qual Life Res 2006] (Cont’d 2)
The same type of instrument may measure different construct[Huang IC, Qual Life Res 2006] (Cont’d 3) † Adjusting for age, gender, educational background, and marriage status
Motivations Does the same domain (e.g., physical functioning) in the SF-36 and the WHOQOL-BREF measure the same construct? Methods Factor analysis Relative validity using different anchors: chronic conditions, health care utilization and global rating of QOL Conclusions The SF-36 and WHOQOL-BREF measures different construct The SF-36 measures the impact of disease / treatment on daily functioning The WHOQOL-BREF measures general satisfaction with life The same type of instrument may measure different constructs[Huang IC, Qual Life Res 2006]
Adopted from the SF-20 HIV/AIDS -specific Disease-specific instrument – MOS-HIV • Development • Albert W. Wu (1993) • Parallel to the MOS SF-36v1 • 10 domains (35 items: 34 +1) • Physical functioning (6 items) • Pain (2 items) • Role functioning (2 items) • Social functioning (1 items) • General health perceptions (5 items) • Energy and fatigue (4 items) • Mental health (5 item) • Cognitive functioning (4 items) • Health distress (4 item) • Quality of life (1 items) • Other: Health transition (1 items) – not used for scoring • Response category • Likert type: 3, 5, or 6 categories
Functioning scales Symptom scales Disease-specific instrument – EORTC QLQ • Development • Neil K. Aaronson (1993) • European Organization for Research and Treatment of Cancer (EORTC) for international clinical trials in oncology • EORTC-QLQ C30: Core questionnaire • Physical functioning (5 items) • Role functioning (2 items) • Social functioning (2 items) • Cognitive functioning (2 items) • Emotional functioning (4 items) • Fatigue (3 items) • Pain (2 items) • Nausea and vomiting (2 items) • Global health status / QOL (2 items) • 6 single items (dyspnoea, loss of appetite, insomnia, constipation, diarrhea and financial loss)
+ EORTC QLQ C-30 Disease-specific instrument – EORTC QLQ (Cont’d) • Response category • Likert type: 4 or 7 categories • Disease or treatment-specific “modules”, e.g., • EORTC QLQ-LC13 (Lung) • EORTC QLQ-BR23 (Breast) • EORTC QLQ-H&N35 (Head & Neck) • EORTC QLQ-OV28 (Ovarian) • EORTC QLQ-CX24 (Cervical) • EORTC QLQ-PR25 (Prostate) • Each module include specific scales, directly relevant to • Disease-related symptoms (e.g., any pain in arm or shoulder) • Morbidity / side effect as a result of specific therapy (e.g., loss of hair, a dry mouth)
Criticism of disease-specific instruments • Over time, some domains may be not imperative due to the introduction of new treatments • For example, the introduction of HAART has changed the survival of HIV/AIDS (from acute to chronic disease) and led to new side effects • Measurement of cognitive (dis)functioning in the MOS-HIV (due to opportunistic infection or AIDS dementia) becomes less important if compared to 10 years ago • Other issue concerning about appearance (facial lipoatrophy due to side effect of treatment) should be included in the measurement
Motivations Should we use generic and / or disease-specific instruments for HRQOL measurement? Methods Diabetes HRQOL using the SF-36 and the D-39 Validating measurement using a variety of clinical measures 1) Lab measure: HbA1c and 2-h postorandial plasma glucose 2) Complication: retinopathy, nephropathy, neuropathy, diabetic foot disorder, cardiovascular and cerebrovascular disorders Findings The SF-36 and D-39 were superior to each other in different regards The SF-36 has superior discriminative validity for complications The D-39 has superior discriminative validity for lab measures Combined use of disease-specific and generic instruments[Huang IC, Value Health 2008]
Direct and indirect health utility measurement • A single index • Value: 0 (worst health) through 1 (best health) • Direct approach (1 stage) • Asking respondents to directly indicate their preference for the health state as one value • Time trade-off (TTO), standard gamble (SG), rating scale (GS) • Indirect approach (2 stages) • Using HRQOL instruments to response their health state and then converting to one utility value using societal preference weights • EQ-5D, Health Utility Index (HUI), SF-6D, Quality of Well-being (QWB)
Perfect health 1.0 Impaired health ? Utility 0 0 Today X Death t (1 yr) Death Time Direct health utility measurement – Time Trade-off • Purpose • Eliciting utility by comparing the value of different health states vs. length of survival • Method • Choices (A): living in a “impaired health state” for time t (e.g., 1 year) • Choice (B): living in a “perfect health state” for time x • Varying time x or t in a systematic fashion to identify the point where subject is indifferent in preference between two scenarios • Health utility = x / t
Perfect health Prob. p Choice (A) Prob. (1-p) Dead Choice (B) Current health state (e.g., cancer) Direct health utility measurement – Standard Gamble • Purpose • Eliciting utility by comparing different choices that account for uncertainty, including risk of death or other outcomes • Method • Choice (A): currently in a specific health state (with symptoms) • Choice (B): a treatment with p% of being perfect health (removing symptoms) and (1-p)% of dead • Varying the probabilities in a systematic fashion to identify the point where subject is indifferent in preference between Choice (A) and (B) • Health utility = p
Indirect health utility measurement – EQ-5D • Development • EuroQol Group (1990) • 5 domains (5 items) • Mobility (1 item) • Usual activities (1 item) • Self-care (1 item) • Pain/discomfort (1 item) • Anxiety/depression (1 item) • Other: one visual analogue scale (0: worst health state; 100: best health state) • Level of health state • 3 levels (no problems, some problems, and severe problems) • Possible health states • 243 (= 3x3x3x3x3)
Indirect health utility measurement – EQ-5D (Cont’d) • Valuation of health states (preference weights) • Protocol: Measurement and Valuation of Health (MVH) • Population: General population in UK [Paul Dolan, Med Care 1997] and in US [Shaw JW, Med Care 2005] • Utility elicitation: using TTO approach for 45 health states and then extrapolating to 243 health states • Scoring system (US): • Health utility for an individual subject (e.g., health state 11223): 1-0-0-0.14-0.173-0.45-(-0.28)-0.011-0-0 = 0.506
Indirect health utility measurement – HUI-3 • Development • George W. Torrance and David Feeny (1990) • Focusing on “within the skin” abilities rather than role performance and social interaction • 8 “attributes” (8 items) • Vision (1 item) • Hearing (1 item) • Speech (1 item) • Ambulation (1 item) • Dexterity (1 item) • Emotion (1 item) • Cognition (1 item) • Pain (1 item) • Level of health states • 5 levels: Speech, emotion, and pain • 6 levels: Vision, hearing, ambulation, dexterity, and cognition
Indirect health utility measurement – HUI-3 (Cont’d) • Possible health states • 972,000 (= 5x5x5x6x6x6x6x6) • Valuation of health states (preference weights) • Population: General population in Canada [Feeny D, Med Care 2002] • Utility elicitation: using RS approach for 73 health states and then extrapolating to 972,000 health states • Scoring system (Canada): • Health utility for an individual subject : 1.371 * (b1 * b2 * b3 * b4 * b5 * b6 * b7 * b8) - 0.371
Crosswalk between health profile and health utility[Huang IC, Health Serv Res 2007] • Motivations • Can we predict health utility using health profiles? • Methods • Using MOS-HIV to predict utility score derived from the EQ-5D
Take home points • How to select instruments? • Conceptual framework of the HRQO/QOL • Characteristics of the population • Purpose of the study (e.g., decision-making at clinical or policy level) • Domains of different instruments with the same label (e.g., physical functioning) may measure different HRQOL/QOL concept • Using qualitative and psychometric approaches (esp., head-to-head comparisons) to elicit instruments genuine properties • Combining generic and disease-specific measures to better capture comprehensive impact of diseases on HRQOL/QOL outcomes